(UroToday.com) At the 2026 PSMA and Beyond annual meeting, Robert Reiter discusses the problems with our PSMA PET reports. Dr. Reiter started by emphasizing that the fundamental problem from a clinician’s perspective is specificity – How do we treat this imaging finding? Is this real? Do we withhold potentially curative treatment based on an imaging finding? Do we over treat a finding that is not cancer? How do we interpret an indeterminate finding? The fundamental problem from a PET physician perspective is sensitivity – we must not miss a lesion, we need to back ourselves up in the case of pursuit, and we are uncertain about what the finding means. How do we communicate this in a way that is helpful to the clinician?
There are several common scenarios to consider:
- Lesions with “low” uptake? True or false positive? Overcalling? Examples include (i) “low” PSMA uptake in a slightly enlarged lymph node(s) in men with newly diagnosed or recurrent prostate cancer, (ii) variable PSMA uptake in one or more rib lesions, and (iii) “low” PSMA uptake in a location not typical for prostate cancer metastasis (ie. mediastinal or inguinal lymph nodes)
- Indeterminate findings - prostate cancer or non-prostate pathology? Examples include (i) “low” or negative PSMA uptake in incidentally found lung nodules, and (ii) uptake in the kidney, pancreas, stomach, and elsewhere
- Discordant findings - true versus false positives? Examples include (i) uptake in a bone lesion without a CT correlate, and (ii) multifocal signal (low to moderate) in the prostate that is discordant with MRI—is this patient a focal therapy candidate or is the secondary uptake signal real?
Dr. Reiter then discussed five specific cases to help illustrate several points. The first case was a 52 year old with Gleason 3+4 on prostate biopsy, and a subsequent PSMA PET that showed:
- Focal low PSMA expression in the left anterior apical gland (SUV max 3.3) likely corresponding to the finding seen on prostate MRI
- Focal low PSMA expression in a small lymph node at the left iliac bifurcation measuring 7 x 10 mm with SUV max 2.7, and PSMA uptake increased on late pelvic acquisition (SUV max 3.8)
- A few sub-centimeter bilateral external iliac lymph nodes with low PSMA uptake are favored reactive.
The impression of the PSMA PET stated “History of prostate cancer with focal low PSMA expression in the left anterior apical gland likely corresponding to findings from prostate MRI and consistent with biopsy-proven prostate malignancy. Low PSMA expression in a small lymph node at the left iliac bifurcation is suspicious for nodal metastasis.” Because of the questionable node in the context of favorable intermediate risk prostate cancer (likely a false positive), the patient opted for a robotic prostatectomy with bilateral pelvic lymph node dissection with the final pathology Gleason 3+4 = 7, pT2N0 (20 lymph nodes). His subsequent PSAs have been < 0.01 ng/mL.
The second case was that of a 58 year old with Gleason 4+3 prostate cancer on biopsy, and a subsequent PSMA PET that showed:
- Focal low PSMA expression slightly increased above background in the right peripheral zone mid gland likely corresponds to the site of previously biopsied tumor.
- Prominent sub-centimeter short axis bilateral external iliac and right inguinal lymph nodes with low PSMA activity, most notable on the delayed phase imaging are indeterminate but suspected reactive given the distribution. Consider follow-up PSMA PET/CT 3 months. Otherwise close attention on follow-up.
- Small region of mild PSMA uptake in the right lateral 6th rib with subtle sclerosis and suggestion of subtle deformity, query healing rib fracture and clinical correlation is suggested.
This report notes the indeterminate lesions, but suggests close attention in follow-up rather than changing therapy. This patient opted for a robotic prostatectomy with bilateral pelvic lymph node dissection with the final pathology Gleason 4+3 = 7, pT2N0 (15 lymph nodes). His subsequent PSAs have been <0.01 ng/mL.
The third case was that of a 70 year old who had previously undergone a robotic prostatectomy in 2019 with Gleason Grade Group 3 prostate cancer pT2N0. Subsequently, he had a biochemical recurrence in 2024 (PSA 0.3 ng/mL) and had salvage radiotherapy to the prostate bed in 2024. The PSA continued to rise to 0.9 ng/mL and he then had a PSMA PET scan:
- History of prostate cancer status post prostatectomy and radiation with no evidence of abnormal PSMA expression in the prostate resection bed to suggest local recurrence.
- No PSMA-avid pelvic lymphadenopathy to suggest nodal metastatic disease.
- The following indeterminate findings:
- Focus of low PSMA expression in the posterior right eighth rib with SUV max 2.2 without definite CT correlate.
- Focus of low PSMA expression in the posterior lateral left seventh rib with SUV max 2.1 without definite CT correlate.
- There is ground glass and soft tissue nodularity measuring up to 8 mm in the left lower lobe with low PSMA expression.
Dr. Reiter notes that this is a challenging scenario, since there is no guidance about the likelihood of true positivity or suitability for biopsy.
The fourth case was that of a 60 year old with Gleason 4+5 = 9 prostate cancer on prostate and a PSMA PET that showed:
- Moderate prostatomegaly with mild to moderate heterogeneous PSMA expression throughout the prostate gland, most pronounced in the right mid gland with SUV max up to 6.1.
- Faint PSMA uptake left lateral second rib is favored benign.
This is an example of a good report suggesting the rib is a false positive, and thus the patient underwent a robotic prostatectomy with pelvic lymph node dissection with final pathology Gleason 4+5 = 9, pT2N0, with PSA follow-up pending.
The fifth and final case was that of a 70 year old s/p cryotherapy with a single MRI PI-RADS 4 lesion, and an initial PSMA PET showing mild uptake bilaterally at the mid gland. Post treatment, the q3 month PSAs were 4.3 4.7 3.8 ng/mL. He subsequently underwent a post-treatment biopsy that was negative for residual cancer. He also had a post-treatment PSMA PET (mandated by a clinical protocol) that showed:
- New, small scattered foci of low PSMA expression in bilateral ribs. At least one lesion is associated with sclerosis and new since prior, concerning for metastatic disease. For example, right posterior rib 4 with SUV max 2.2.
- Nonspecific, low to intermediate PSMA expression in the prostate more prominent in the left posterolateral peripheral midgland and apex.
Dr. Reiter notes that this is a challenging report to interpret given that the suggestion of metastasis seems inconsistent with the clinical history.
Dr. Reiter concluded his presentation discussing the problems with our PSMA PET reports with the following solutions for improving reporting:
- Explicitly list size and PSMA PET signal of indeterminate lesions
- Provide an opinion of low or high suspicion to help guide clinician—avoid vagueness whenever possible
- Provide differential diagnosis given the context of the patient’s history (when available)
- Suggest actions when possible, such as confirmatory biopsy or imaging
- Suggest multidisciplinary discussion
- Communication between treating physician and nuclear medicine/radiologist
- Use standardized and structured reporting (Primary, Promise, Promise V2), but:
- We need integration of standard reporting features of lesions with interpretation needed for clinical care
- Requires education of clinicians
- There are very few that are familiar with PRIMARY or PRIMARY v2, thus education is needed to make this scoring system similar to the PI-RADS reporting for mpMRI
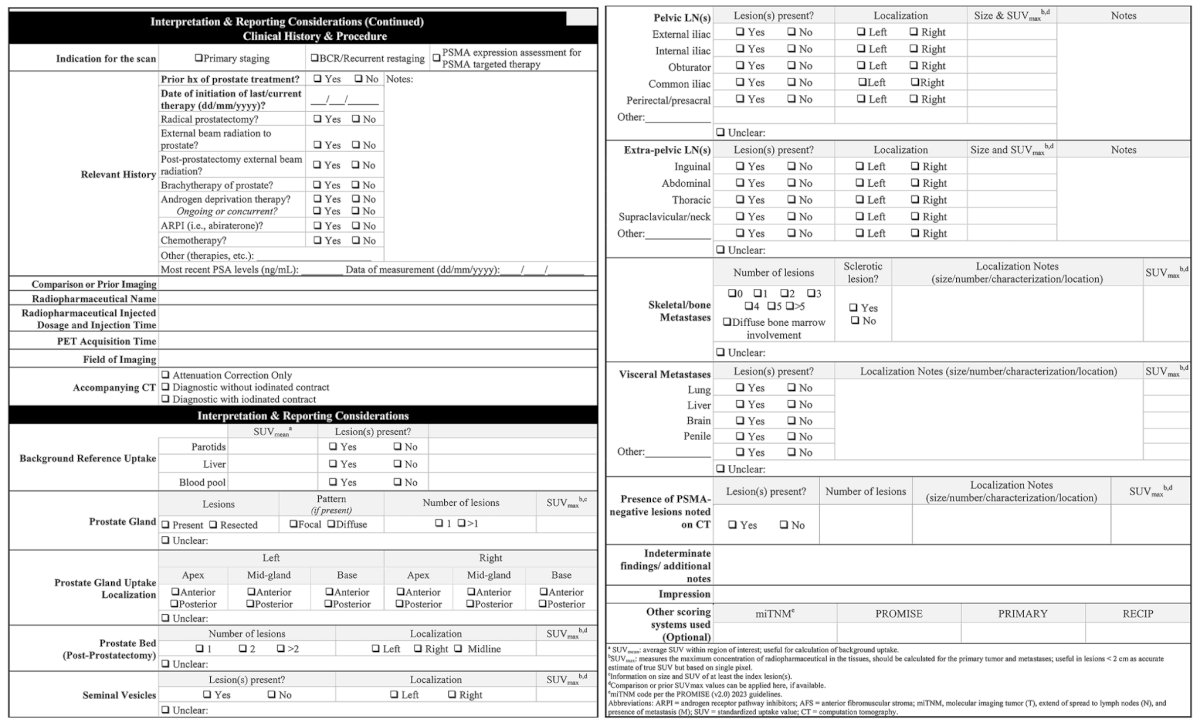
There are several standardized templates for reporting PSMA PET/CT scans, including the following provided by Esfahani et al. [1]:
Presented by: Robert Reiter, MD, University of California – Los Angeles, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 PSMA & Beyond Conference, Los Angeles, CA, Thurs, Mar 26 – Fri, Mar 27, 2026.
Related content: The Problem with Our Reports "Presentation" - Robert Reiter
References: