(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a new developments in genitourinary radioligand therapy session and a presentation by Dr. Brian Shuch discussing CA-IX in renal cell cancer (RCC). Secondary to 43% of Medicare patients having a CT of the chest/abdomen within 5 years, this has led to an increase in detection of 2-4 cm tumors. As such, there has also been a stage migration for RCC, with 70% of RCC cases now cT1, and 4x more kidney operations performed than in the 1970’s. However, 30% of small renal masses at diagnosis are benign at the time of surgery. Importantly 0.2% of patients will die < 90 days after an RCC operation.
Although there are 15+ subtypes, 63% of RCC are clear cell, with 90% of deaths attributed to clear cell RCC. On surveillance, clear cell RCC has the fastest growth rate when compared to papillary RCC or chromophobe RCC, as well as earlier rates of metastasis.
Dr. Shuch discussed the limitations of conventional imaging, one of which is that enhancement does not equal cancer, and cancer does not equal aggressiveness. However, enhancement patterns may suggest specific histology. In the REDECT trial,1 brisk enhancement showed a sensitivity of 75.5% and specificity of 47% for clear cell RCC, whereas low/delayed enhancement had a sensitivity of 70% and specificity of 85% for papillary RCC. There are several new approaches, including the UTSW, CCLS, and UCLA scores, which suggest sensitivities and specificities of 75-80%.
Regarding renal mass biopsy, there are several limitations, including:
- Error: biopsies are invasive and subject to sampling errors
- Insufficient tissue: 10-15% of cases are non-diagnostic
- NPV is ~70% for core biopsies
- Tumor seeding: may occur in the biopsy tract in 1.2% of biopsies
- Upstaging to pT3 disease is increased in those undergoing a biopsy
- Complications: hematoma (4.9%), significant pain (1.2%), gross hematuria (1.0%), pneumothorax (0.6%), and hemorrhage (0.4%)
For FDG PET/CT, there is uptake/physiological urinary excretion of FDG, with often similar FDG levels in the lesions as compared to urine and renal parenchyma. Some benign renal lesions will also be metabolically active:

CA-IX shows diffuse membrane staining in clear cell RCC, as well as focal CA-IX staining in papillary RCC. Starting in 1986, there has been a long journey for CA-IX clinical development:

Girentuximab is a IgG1 kappa light chain chimeric monoclonal antibody that binds with high specificity to CA-IX and is internalized. Hepatobiliary excretion allows optimal renal visualization, and various payloads can be attached. Additionally, imaging is feasible with both PET/CT and SPECT/CT, with extensive experience in prior imaging and therapeutic studies. The REDECT trial was an open-label multicenter study of 124I-girentuximab PET/CT in 195 patients with renal masses who were scheduled for resection. The mean sensitivity was 86.2% (95% CI, 75.3% to 97.1%) for PET/CT and 75.5% (95% CI, 62.6% to 88.4%) for contrast enhanced CT (p = 0.023), and the mean specificity was 85.9% (95% CI, 69.4% to 99.9%) for PET/CT and 46.8% (95% CI, 18.8% to 74.7%) for contrast enhanced CT (p = 0.005). However, the study was underpowered and Wilex shut down the isotope after a negative adjuvant trial.
Dr. Shuch then discussed the ZIRCON trial,2 which was initially presented at ASCO GU 2023. ZIRCON was an open-label, multicenter clinical trial, recruiting patients with an indeterminate renal masses (≤ 7 cm; tumor stage cT1) who were scheduled for partial nephrectomy within 90 days from planned TLX250-CDx administration. Enrolled patients received a single dose of TLX250-CDx IV (37 MBq ± 10%; 10 mg girentuximab) on Day 0 and underwent PET/CT imaging on Day 5 (± 2 days) prior to surgery:
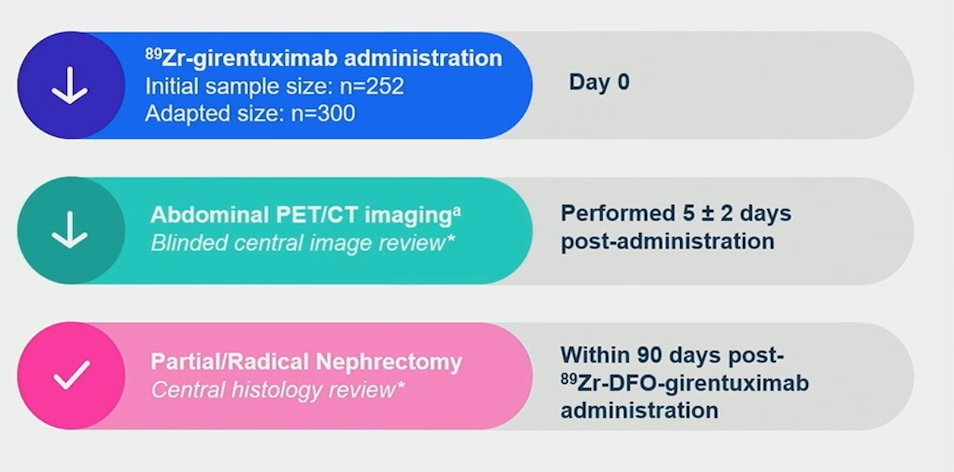
Blinded central histology review determined clear cell RCC status. The co-primary objectives were to evaluate both the sensitivity and specificity of TLX250-CDx PET/CT imaging in detecting clear cell RCC in patients with indeterminate renal masses, using histology as the standard of truth. Key secondary objectives included sensitivity and specificity of TLX250-CDx PET/CT imaging in the subgroup of patients with indeterminate renal masses ≤ 4 cm (cT1a). Other secondary objectives included positive and negative predictive values, safety, and tolerability.
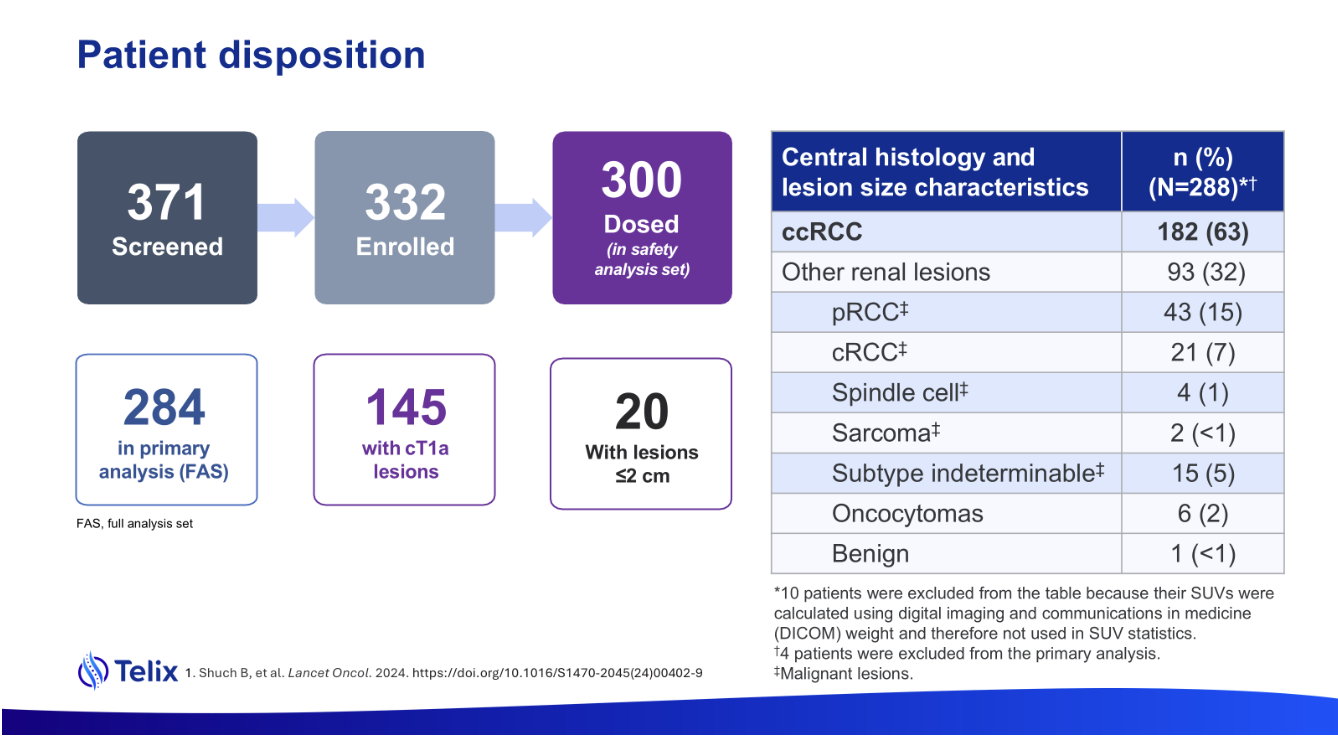
There were 332 patients (300 in the safety analysis) enrolled between August 2019 and August 2022 among 36 sites in 9 countries that received TLX250-CDx. The median age was 62 years (range: 27-87), and 71.3% of patients were male. Of 288 patients with central histopathology of surgical samples, 193 (67%) had clear cell RCC. Based on central review, 51% had cT1a disease, and 7% of tumors measured ≤2 cm:
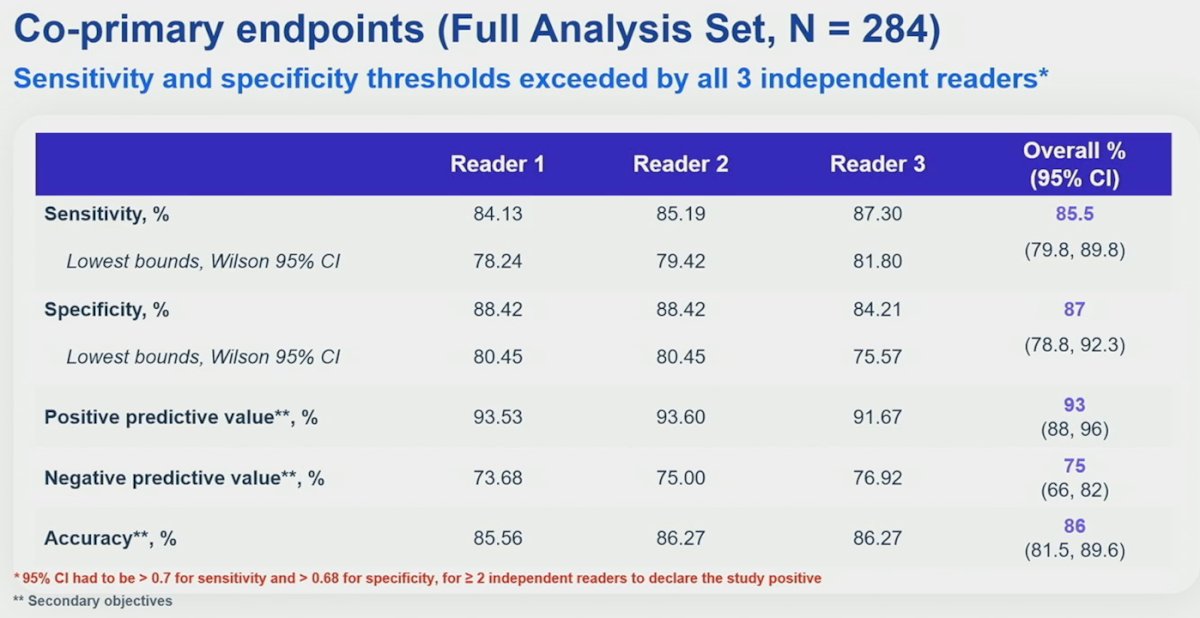
Of 284 evaluable patients included in primary analysis, the average across all 3 readers for sensitivity and specificity was 86% [95% CI 80%, 90%] and 87% [95% CI 79%, 92%], respectively, for co-primary endpoints, and 85% [95% CI 77%, 91%] and 90% [95% CI 79%, 95%], respectively, for key secondary endpoints. For all readers, the lower boundaries of 95% CI for co-primary and key secondary endpoints were > 75%. In the intention-to-treat population, the positive predictive value was 93% and the negative predictive value was 75%.
On February 26, 2025, the FDA accepted the BLA for TLX250-CDx, which was granted a priority review and provided a PDUFA date of August 27, 2025.
Since the ZIRCON trial, there has been a 89Zr-DFO-girentuximab expanded access program, allowing 102 patients to be dosed and imaged. Of note, the majority of sites enrolling patients in the expanded access program were not sites participating in ZIRCON.
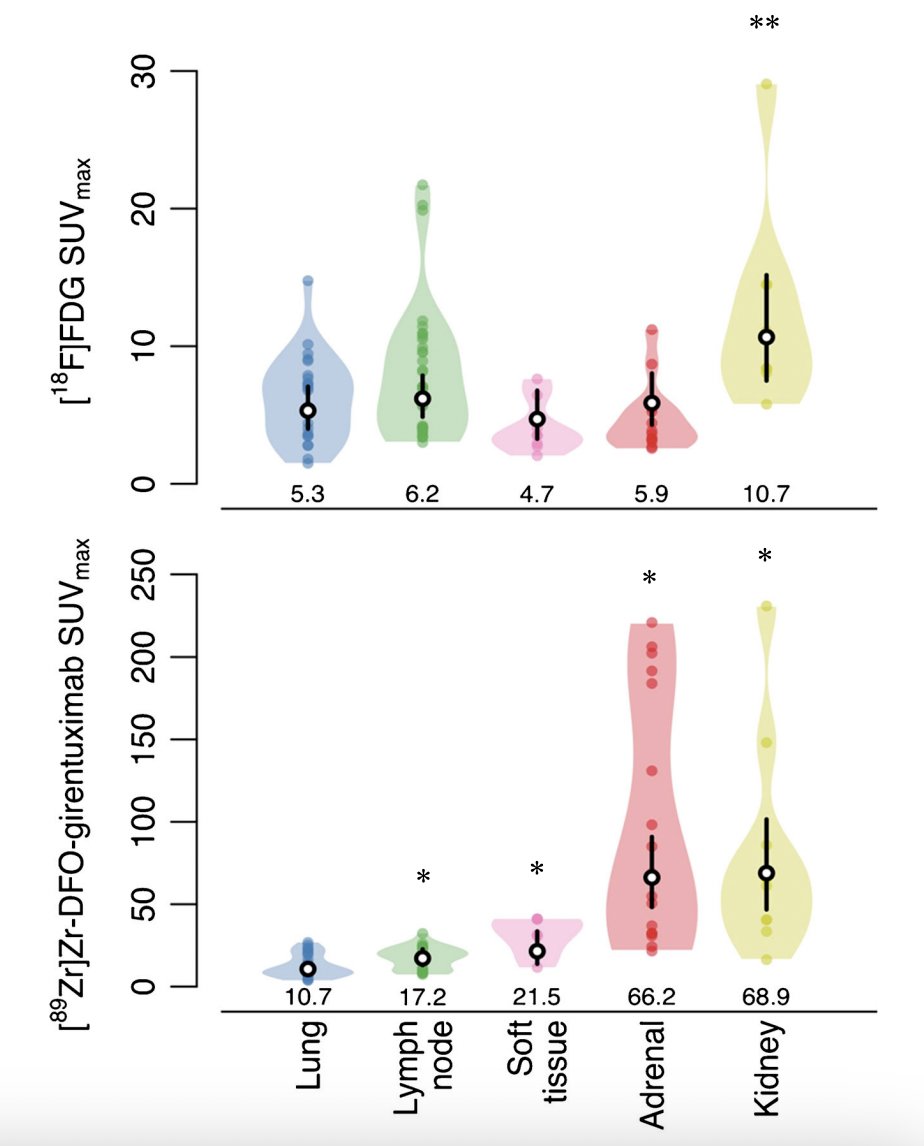
Next, Dr. Shuch discussed imaging of metastatic disease. In 2019, the Impact-RCC trial was published, which was a study evaluating the lesion detection of baseline contrast-enhanced CT, [89Zr]Zr-DFO-girentuximab-PET/CT and [18F]FDG-PET/CT in detecting clear cell RCC lesions in 42 patients with a good or intermediate prognosis metastatic clear cell RCC according to the IMDC risk model. A total of 449 lesions were detected by ≥1 modality (median per patient: 7) of which 42% were in lung, 22% in lymph nodes and 10% in bone:
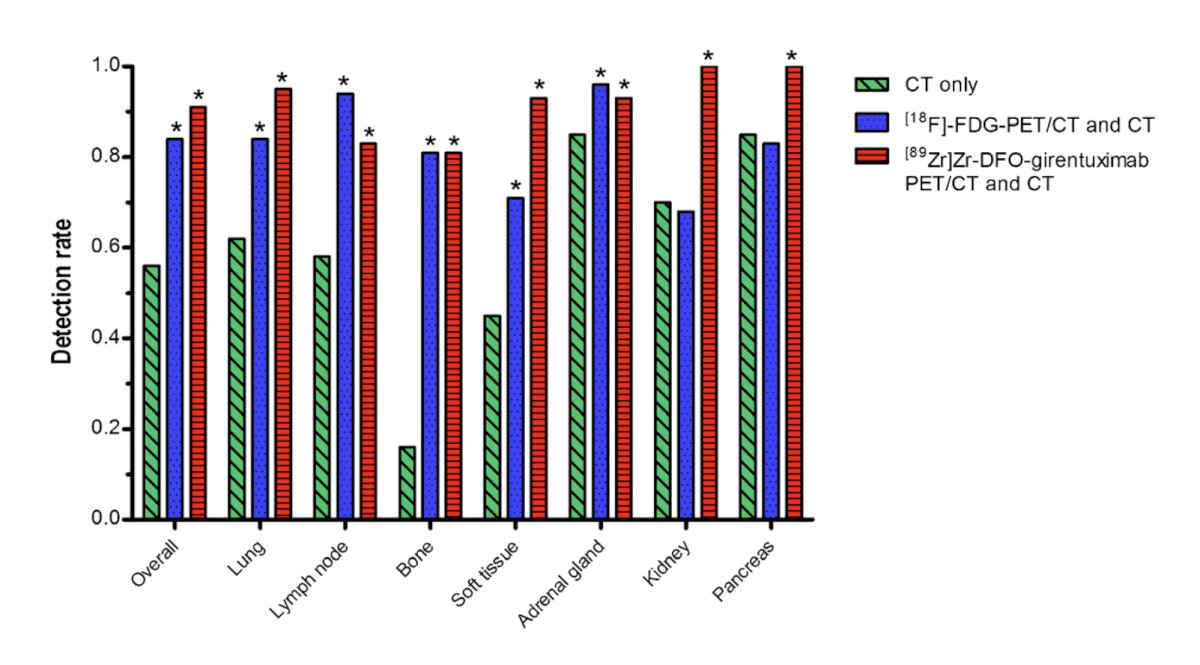
Combined [89Zr]Zr-DFO-girentuximab-PET/CT and CT detected more lesions than CT alone: 91% (95% CI 87-94) versus 56% (95% CI 50-62, p = 0.001), respectively, and more than CT and [18F]FDG-PET/CT combined (84% (95% CI 79-88, p < 0.005). The following Violin plot shows the actual distribution of [89Zr]Zr-DFO-girentuximab-PET/CT and [18F]FDG-PET/CT SUVmax in tumor lesions per organ site:
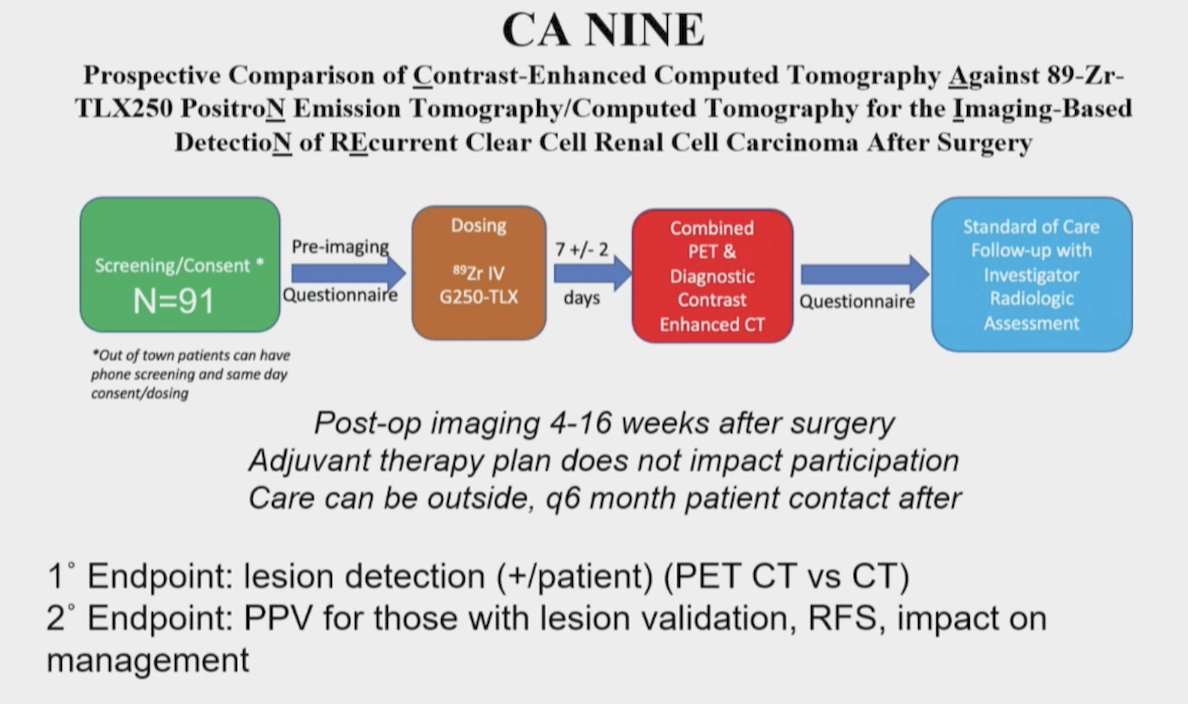
Dr. Shuch and Dr. Calais have opened the CA NINE trial, which is a prospective comparison of contrast-enhanced CT against 89Zr-TLX250 PET for the imaging-based detection of recurrent clear cell renal cell carcinoma after surgery. Current enrollment in this trial is 13 patients:
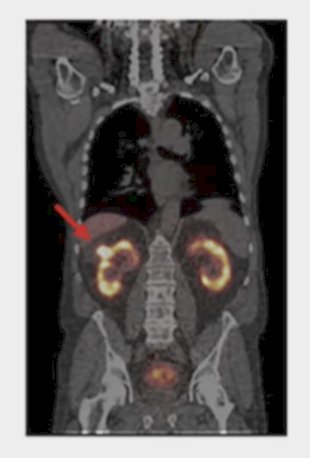
Dr. Shuch finished his discussion by highlighting two small molecules that are in development for PET/CT imaging. The first is DPI-4452, in which 68Ga-DPI-4452 (a CA-IX binding peptide) is theranostically paired with 177Lu-DPI-4452 and used to treat 3 patients with metastatic clear cell RCC treated with 2+ prior lines of therapy. There were no adverse events, with very high background biliary/gastric uptake, and low kidney background signal. The second is PHC-102, which is an acetazolamide analogue that was injected into 5 patients with localized or metastatic clear cell RCC. Similarly, there were no adverse events, biliary/gastric uptake was expected, but with renal clearance and high kidney background. Despite renal clearance, there is still appreciable delineation of the RCC:
Dr. Shuch concluded his presentation discussing CA-IX in RCC with the following take home points:
- Overtreatment and undertreatment are both problems in RCC due to the significant limitations with conventional imaging and biopsy
- CA-IX is expressed in clear cell RCC and some hypoxic non clear cell RCC
- Antibody and small molecule radiotracers are in clinical development for CA-IX-based imaging
- The TLX250-CDx biologic license application is to be reviewed in the summer of 2025
- Identification of metastatic disease and theranostic approaches are being actively investigated in kidney cancer and beyond
Presented by: Brian Shuch, MD, University of California, Los Angeles, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Divgi CR, Uzzo RG, Gatsonis C, et al. Positron emission tomography/computed tomography identification of clear cell renal cell carcinoma: Results form the REDECT trial. J Clin Oncol. 2013 Jan 10;31(2):187-194.
- Shuch B, Pantuck AJ, Bernhard JC, et al. [89Zr]Zr-girentuximab for PET-CT imaging of clear-cell renal cell carcinoma: A prospective, open-label, multicentre, phase 3 trial. Lancet Oncol. 2024 Oct;25(10):1277-1287.
- Verhoeff SR, van Es SC, Boon E, et al. Lesion detection by. [89Zr]Zr-DFO-girentuximab and [18F]FDG-PET/CT in patients with newly diagnosed metastaic renal cell carcinoma. Eur J Nucl Med Mol Imaging. 2019 Aug;46(9):1931-1939.