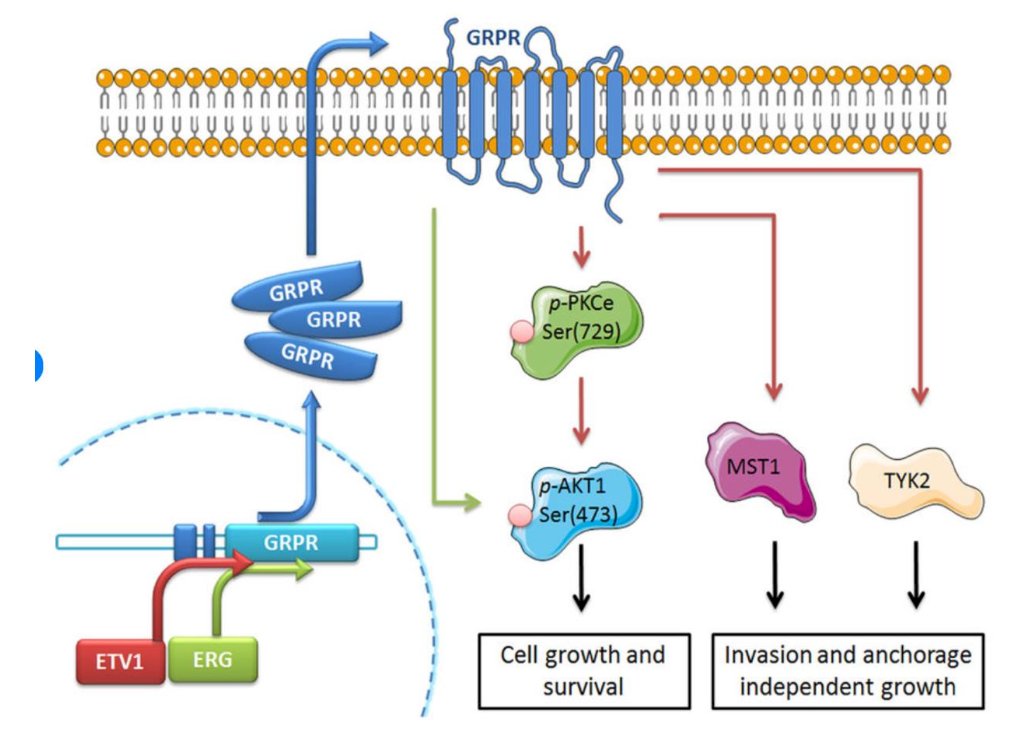
(UroToday.com) The 2025 PSMA and Beyond annual meeting featured new developments in genitourinary radioligand therapy session and a presentation by Dr. Andrei Iagaru discussing GRPR and other peptides for targeting prostate cancer. PSMA is a transmembrane protein overexpressed in prostate cancer, which has known enzymatic activities and acts as a glutamate-preferring carboxypeptidase. Gastrin releasing peptide receptor (GRPR) is a G-protein-coupled receptor overexpressed in a variety of major human cancers, such as prostate, breast, small cell lung cancers, and tumors of the urinary tract:
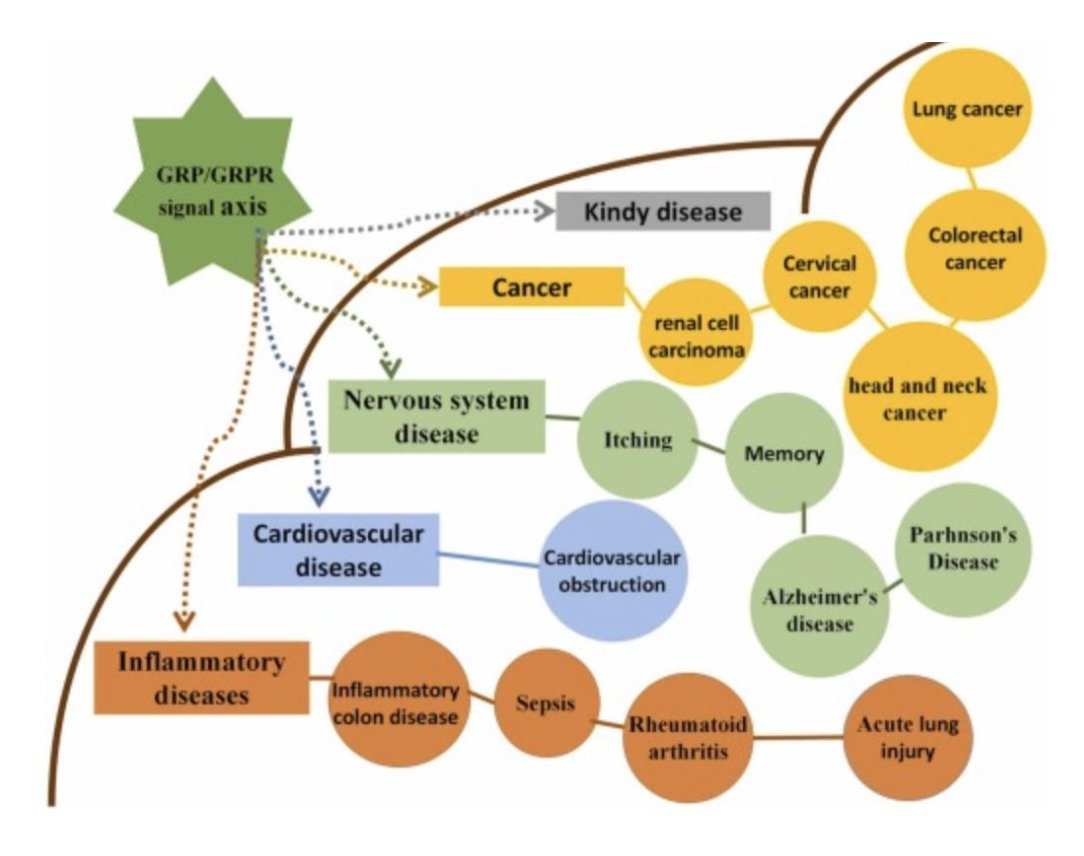
The GRPR signaling axis is involved in many pathophysiological aspects, including kidney disease, nervous system disease, cardiovascular disease, inflammatory disease, and cancer:
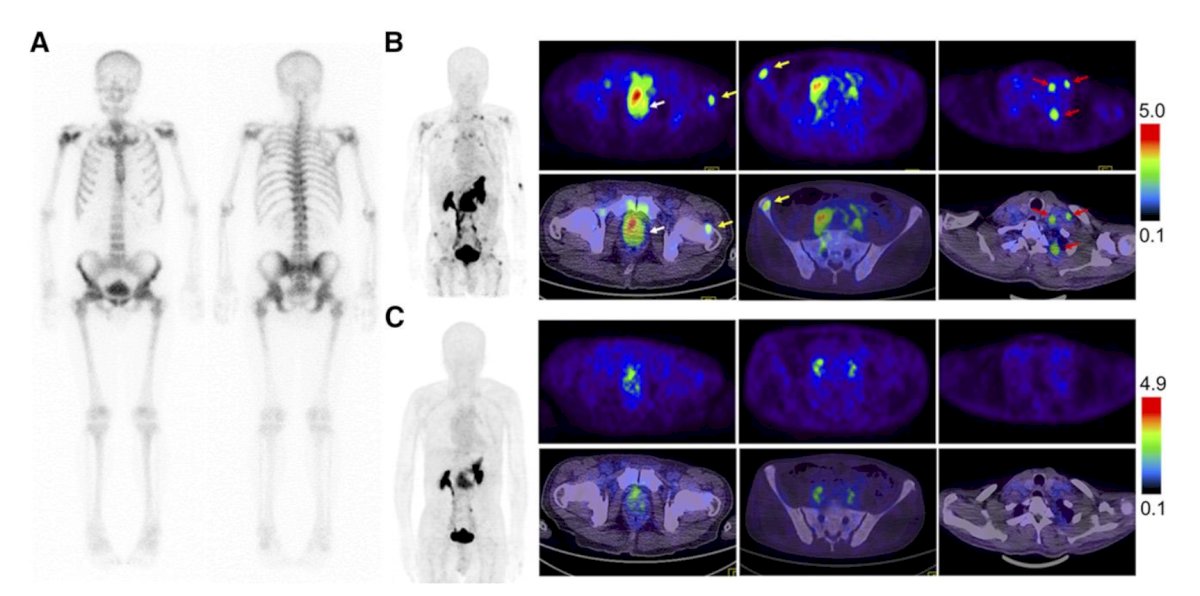
In 2018, Zhang and colleagues1 assessed 68Ga-RM26 in 5 healthy volunteers and 28 patients with prostate cancer noting that 68Ga-M26 was well tolerated by all subjects, with no adverse symptoms reported during the procedure and at 2 week follow-up. In the 17 patients with newly diagnosed prostate cancer, 68Ga-RM26 PET/CT showed positive prostate-confined findings in 15 tumors with an SUVmax of 6.49 ± 2.37. In the 11 patients who underwent prostatectomy or brachytherapy with or without ADT, 68Ga-RM26 PET/CT detected 8 metastatic lymph nodes in 3 patients with an SUVmax of 4.28 ± 1.25 and 21 bone lesions in 8 patients with an SUVmax of 3.90 ± 3.07:
Previous in vivo work suggests that 177Lu-RM2 therapy is effective as a single agent, however, there is further improved efficacy with combination therapy of 177Lu-RM2 and rapamycin.
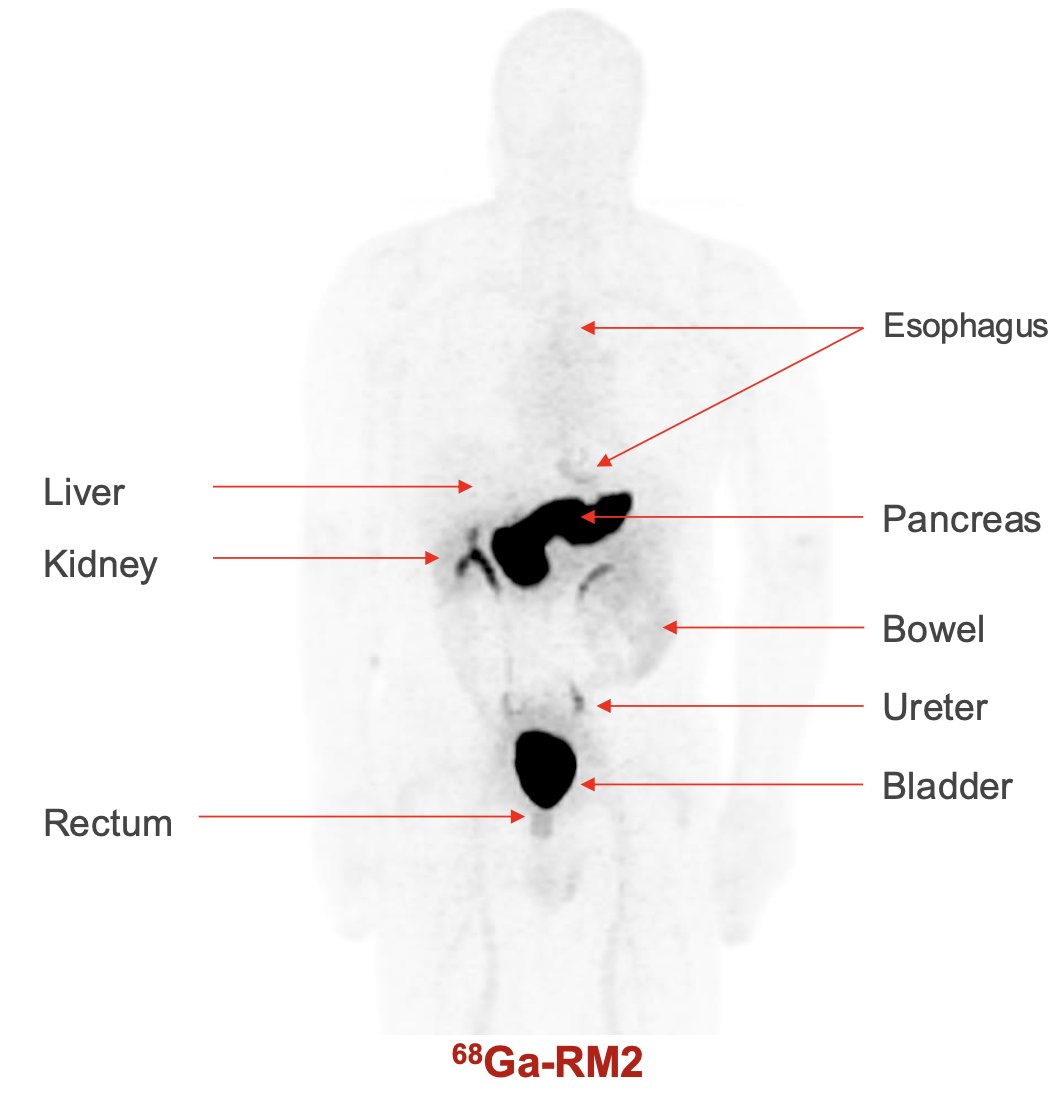
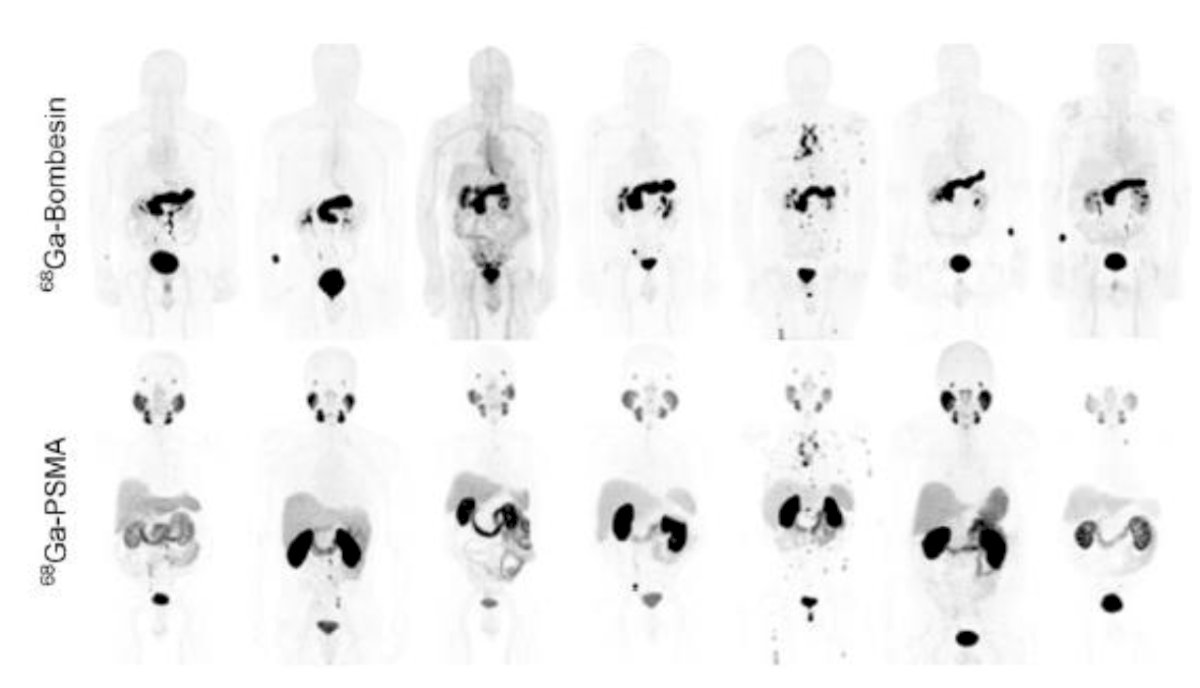
Next, Dr. Iagaru discussed the Stanford experience with GRPR PET (2015 – present). Normal biodistribution of 68Ga-RM2 includes the esophagus, liver, pancreas, kidney, bowel, ureter, bladder, and rectum:
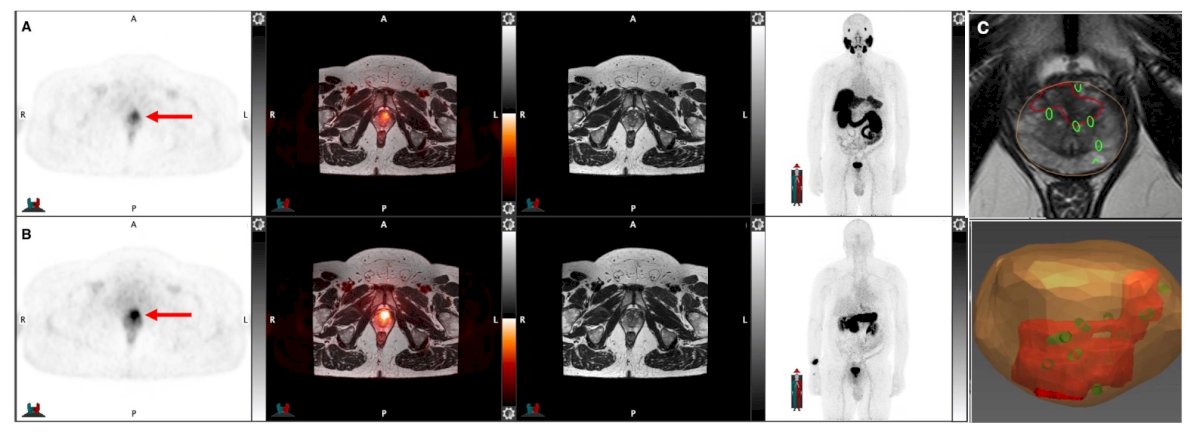
In a pilot study by Dr. Iagaru’s group of 68Ga-PSMA-11 and 68Ga-RM2 PET/MRI for biopsy guidance in 13 patients suspected of prostate cancer,2 68Ga-PSMA11 identified 25 lesions, of which 11 (44%) were true-positive (5 with clinically significant prostate cancer). 68Ga-RM2 showed 27 lesions, of which 14 (52%) were true positive, identifying all 7 cases of clinically significant prostate cancer and also 7 with non-clinically significant prostate cancer. There were 17 concordant lesions in 11 patients versus 14 discordant lesions in 7 patients between 68Ga-PSMA11 and 68Ga-RM2 PET:
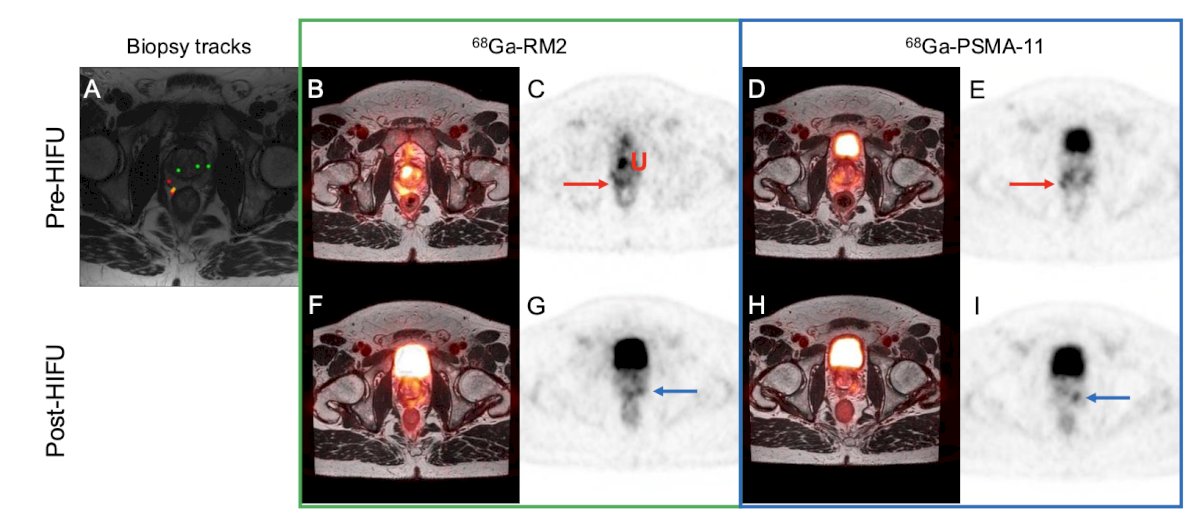
In another study from his group,3 they assessed a pilot study of 68Ga-PSMA-11 and 68Ga-RM2 PET/MRI for evaluation of prostate cancer response to high-intensity focal ultrasound (HIFU) therapy. Among 14 patients, 68Ga-PSMA11 and 68Ga-RM2 PET/MRI each showed 23 positive intraprostatic lesions: 21 were congruent in 13 patients, and 5 were incongruent in 5 patients. Before HIFU, 68Ga-PSMA11 identified all target tumors, whereas 68Ga-RM2 PET/MRI missed 2 tumors. After HIFU, 68Ga-RM2 and 68Ga-PSMA11 PET/MRI both identified clinically significant residual disease in 1 patient:
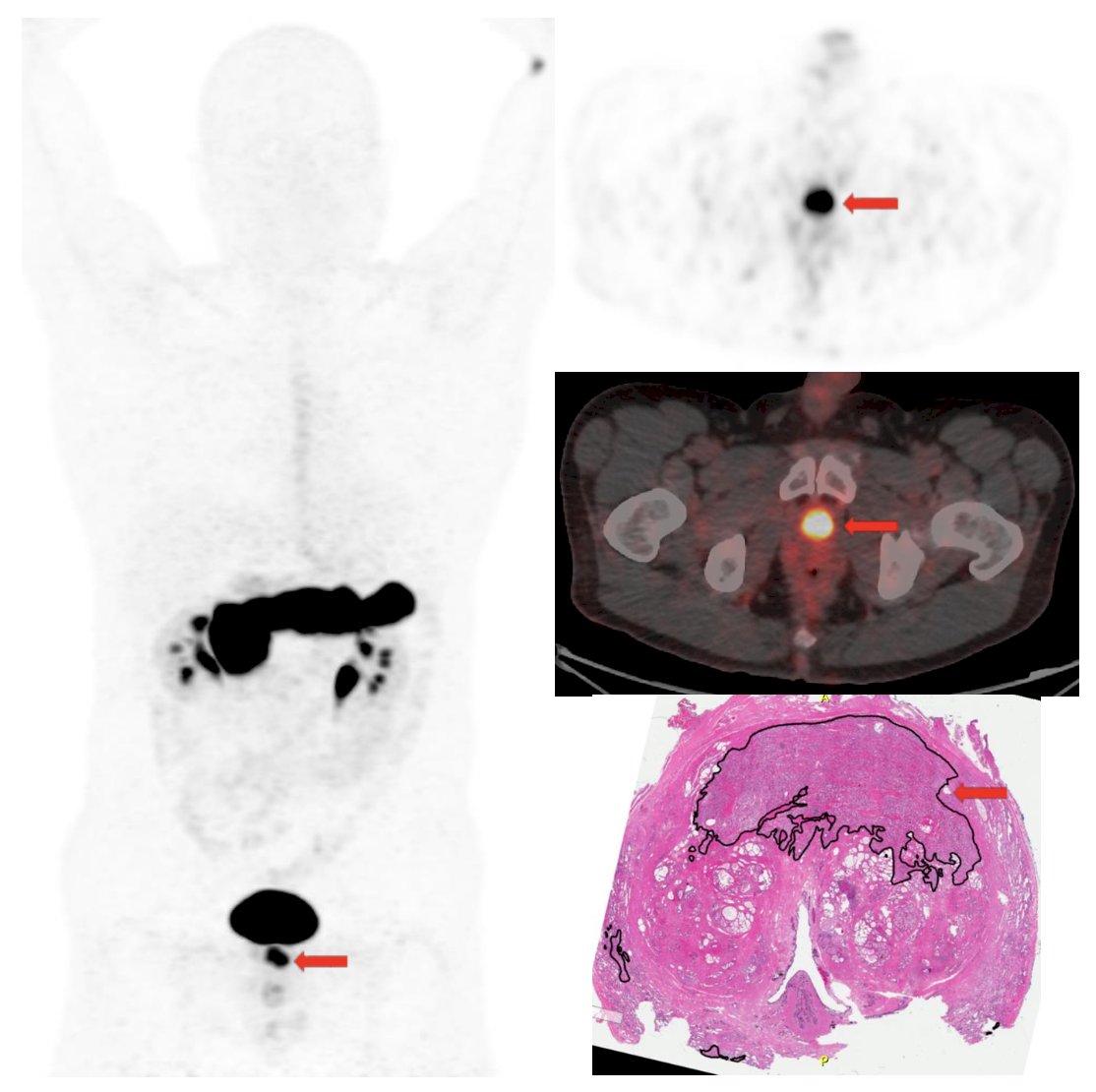
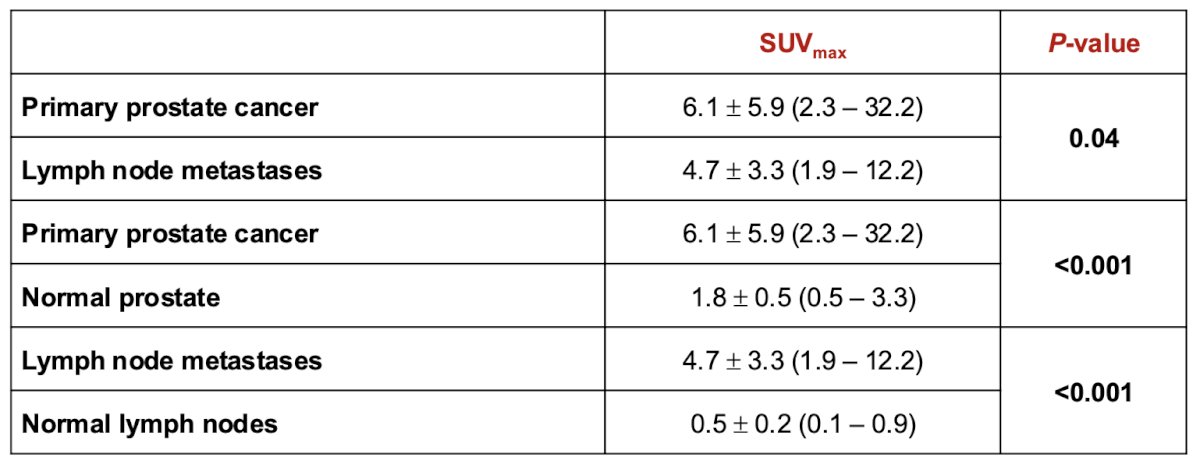
In a third study from Dr. Iagaru’s group,4 they assessed the correlation of 68Ga-RM2 PET with post-surgery histopathology findings in patients with newly diagnosed intermediate- or high-risk prostate cancer. Among 41 men, preoperative 68Ga-RM2 PET identified 70 intraprostatic foci of uptake in 40 of 41 patients. Post-prostatectomy histopathology was available in 32 patients in which 68Ga-RM2 PET identified 50 of 54 intraprostatic lesions (detection rate 93%). 68Ga-RM2 uptake was recorded in 19 non-enlarged pelvic lymph nodes in 6 patients, pathology confirmed lymph node metastases in 16 lesions, and follow-up imaging confirmed nodal metastases in 2 lesions:
The results for SUVmax are noted in the following table:
In 2016, Minamimoto et al.5 reported a pilot comparison of 68Ga-RM2 PET and 68Ga-PMSA-11 PET in 7 patients with biochemically recurrent prostate cancer. Uptake outside the expected physiologic biodistribution did not significantly differ between 68Ga-PMSA-11 and 68Ga-RM2, however, 68Ga-PMSA-11 localized in a lymph node and seminal vesicle in a patient with no abnormal 68Ga-RM2 uptake. Abdominal periaortic lymph nodes were more easily visualized by 68Ga-RM2 in two patients because of a lack of interference by radioactivity in the small intestine:
In 2024, Dr. Iagaru’s group reported results of a single-center, single-arm, phase 2/3 imaging trial of 68Ga-RM2 PET-MRI versus MRI alone for evaluation of 100 patients with biochemical recurrence of prostate cancer.6 Over a median follow-up of 49.3 months (IQR 36.7-59.2), 68Ga-RM2 PET-MRI was positive in 69 (69%) patients and MRI alone was positive in 40 (40%) patients (p < 0.0001). In the per-lesion analysis 68Ga-RM2 PET-MRI showed significantly higher detection rates than MRI alone (143 versus 96 lesions; p < 0.0001). The positivity rates stratified baseline PSA are as follows, noting a 40.7% positivity rate with a PSA < 0.5 ng/mL:

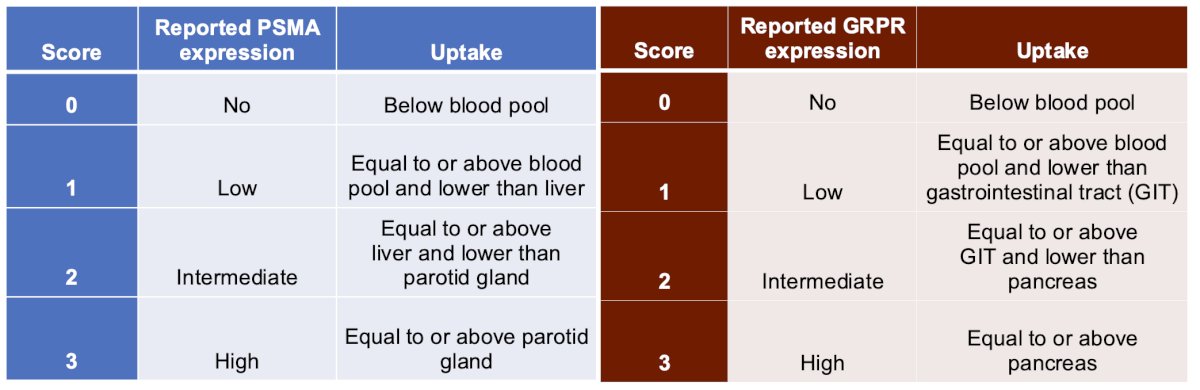
Next, Dr. Iagaru discussed standardized interpretation of GRPR PET using a modified PROMISE criteria, with the following reporting table compared to PSMA expression:7
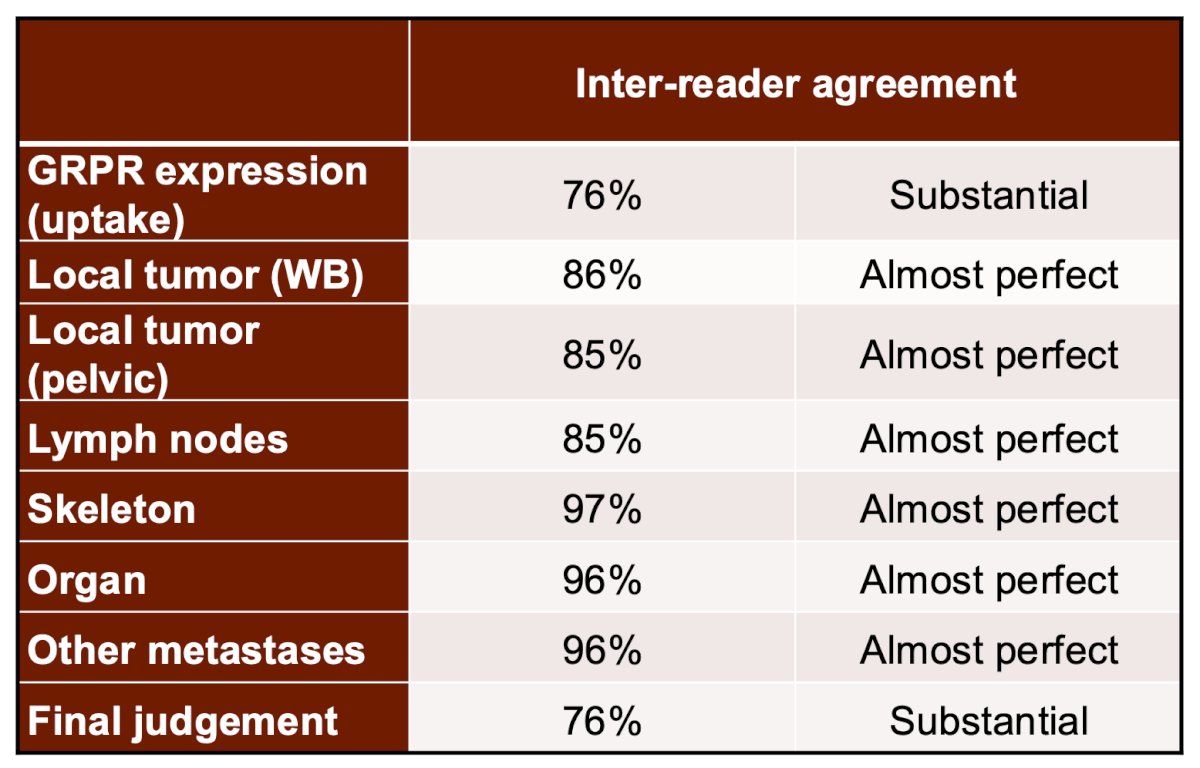
Inter-reader agreement for GRPR PET imaging is highlighted below:
Dr. Iagaru finished his presentation discussing several future directions in this disease space. 64Cu SAR-Bombesin has developed a radioisotope for men with biochemically recurrent prostate cancer:

Koller and colleagues8 previously reported a preclinical comparison of the 64Cu- and 68Ga-labeled GRPR-targeted compounds RM2 and AMTG. They found that overall biodistribution profiles and tumor-to-background ratios were comparable but slightly enhanced for the 68Ga-labeled analogs in most organs. The following image is of a patient with mCRPC after four cycles of 177Lu-PSMA-617 radioligand therapy with multiple peri-hepatic and abdominal lymph node metastases that currently show no or only faint uptake on 18F-PSMA-1007 PET/CT, but intense uptake on 68Ga-AMTG PET/CT:

Dr. Iagaru notes that procedure standardization is the next milestone for GRPR theranostics and a standardized PET image has been proposed, the mPROMISE criteria. These criteria can be used to select patients for GRPR theranostics, with tumor uptake higher than the gastrointestinal tract and pancreas being key criteria to ensuring the best patient outcomes. GPRP-targeted radiopharmaceuticals hold high promise for staging, restaging, and treatment of GRPR expressing cancer, primarily prostate cancer and breast cancer, the most common cancers in men and women, respectively.
Dr. Iagaru concluded his presentation discussing GRPR and other peptides for targeting prostate cancer with the following take home points:
- Great progress has been made in the last 10+ years establishing the foundations for future developments, including GRPR PET interpretation criteria
- We need to move from small cohorts to well designed, large, multi-center prospective studies with defined indications
- More investigators/pharma should think beyond PSMA, given complex prostate cancer biology, no matter how excellent PSMA is
- Identification of appropriate clinical scenarios for the use of GRPR is important, as the late stage is too late
- Our goal should be to have at least 1 GRPR theranostic pair FDA-approved for therapy in the next decade
Presented by: Andrei Iagaru, MD, Stanford University, Palo Alto, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Zhang J, Niu G, Fan X, et al. PET using a GRPR antagonist 68Ga-RM26 in healthy volunteers and prostate cancer patients. J Nucl Med. 2018 Jun;59(6):922-928.
- Duan H, Ghanouni P, Daniel B, et al. A pilot study of 68Ga-PSMA-11 and 68Ga-RM2 PET/MRI for biopsy guidance in patients suspected of prostate cancer. J Nucl Med. 2023;64(5):744-750.
- Duan H, Ghanouni P, Daniel B, et al. A pilot study of 68Ga-PSMA-11 and 68Ga-RM2 PET/MRI for evaluation of prostate cancer response to high-intensity focal ultrasound therapy. J Nucl Med. 2023;64(4):592-597.
- Duan H, Baratto L, Fan RE, et al. Correlation of 68Ga-RM2 PET with postsurgery histopathology findings in patients with newly diagnosed intermediate- or high-risk prostate cancer. J Nucl Med. 2022;63(12):1829-1835.
- Minamimoto R, Hancock S, Schneider B, et al. Pilot comparison of 68Ga-RM2 PET and 68Ga-PMSA-11 PET in patients with biochemically recurrent prostate cancer. J Nucl Med. 2016 Apr;57(4):557.562.
- Duan H, Moradi F, Davidzon GA, et al. 68Ga-RM2 PET-MRI versus MRI alone for evaluation of patients with biochemical recurrence of prostate cancer: A single-center, single-arm, phase 2/3 imaging trial. Lancet Oncol. 2024 Apr;25(4):501-508.
- Eiber M, Herrmann K, Calais J, et al. Prostate cancer molecular imaging standardized evaluation (PROMISE): Proposed miTNM classification for the interpretation of PSMA-ligand PET/CT. J Nucl Med. 2018;59(3):469-478.
- Koller L, Joksch M, Schwarzenbock S, et al. Preclinical comparison of the 64Cu- and 68Ga-labeled GRPR-targeted compounds RM2 and AMTG, as well as first-in-humans [68Ga]-Ga-AMTG PET/CT. J Nucl Med. 2023 Oct;64(10):1654-1659.