(UroToday.com) The 2025 PSMA and Beyond annual meeting featured an alpha and other radionuclides session and a presentation by Dr. Sue Yom discussing the management of dry mouth. Saliva has many types and sources, including:
- Parotid glands:
- Secretions are purely serous
- Produces most saliva output during eating (“stimulated saliva”)
- Submandibular glands and sublingual glands:
- Secretions contain mucins, which are glycoproteins that adhere to oral mucosal surfaces and absorb water, providing a sense of hydration
- Produce most of the saliva while not eating (“resting saliva”)
- Minor salivary glands of the oral cavity: produce most of the salivary mucins
The consequences of dry mouth are (i) poor sleep, (ii) daytime bother, (iii) difficulty chewing, swallowing, and speaking, (iv) fungal and bacterial infections, (v) candidiasis, (vi) impaired taste, (vii) enamel erosion and dental caries, (viii) gingivitis and periodontitis, and (ix) poor nutrition.
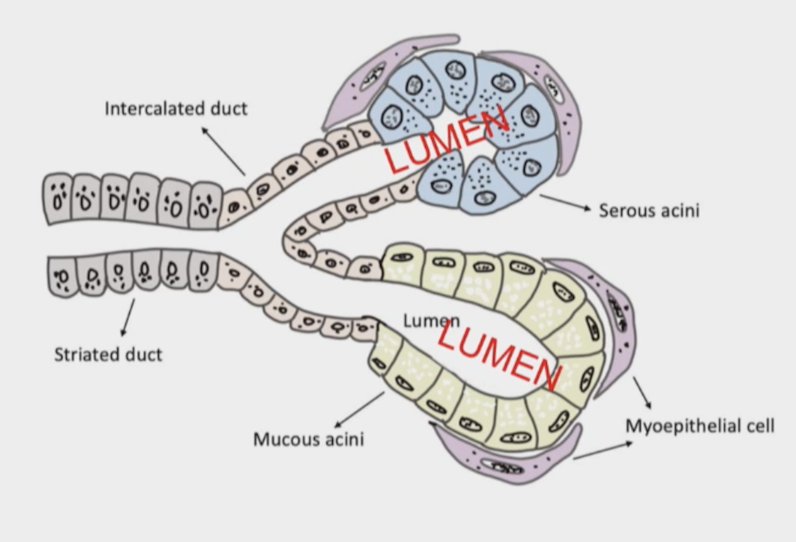
Dr. Yom notes that PSMA is expressed on the apical lumen of the acinar epithelium in human salivary glands, and acinar epithelium is sensitive to ionizing radiation, with poor regenerative capacity. Glutamate carboxypeptidase III may be another mechanism for the accumulation of PSMA in salivary tissue:
There is a proven dose response of xerostomia, with a mean dose of 40 Gy conferring a 50% risk of reducing flow by 75% at 1 year. However, a mean of 26 Gy (17-26% risk) is commonly used as a dose limit in planning IMRT. In the VISION1 trial, 6 cycles of 177Lu-PSMA-617 led to a cumulative absorbed dose of 28 Gy to the salivary glands.
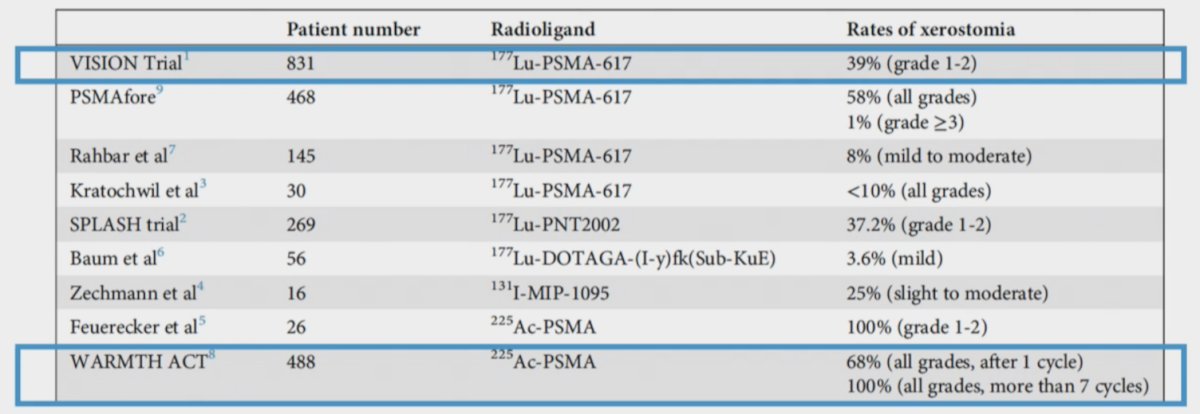
In a recent article from Pepin et al.2, they note that rates of xerostomia in the VISION trial were 39% grade 1-2, whereas the WARMTH ACT3 trial showed 68% all grade rate after 1 cycle, and 100% all grade rate after more than 7 cycles of 177Lu-PSMA-617:
Dr. Yom notes that prevention via blockade is from vasoconstriction or competitive uptake. This can be done via:
- Cooling: trial of ice packs on the right parotid gland replaced every 30 minutes for 4 hours
- Botulinum injection: only case reports
- MSG oral ingestion: a placebo controlled trial showed a median decreased uptake of 33%, but also a corresponding reduced PSMA tumor uptake
The radioprotectant amifostine reduces radiation related grade 3-4 mucositis, requiring on site administration within 30 minutes, but also being associated with difficult side effects (nausea, hypotension). There are also concerns about protecting the tumor from therapy. There are also a number of other radioprotectants that are being evaluated and mostly aimed at mucositis:
- Palifermin: binds keratinocyte growth factor receptor
- Showed reduced grade 3-4 oral mucositis in a phase III study of head and neck chemoradiation
- Not approved due to lack of improvement in narcotic use, pain, or therapy tolerance
- GC4419: mimetic of antioxidant superoxide dismutase
- Granted Fast Track and Breakthrough Therapy designations by the FDA for severe oral mucositis induced by radiotherapy with or without therapy
- Was not approved due to lack of clinical impact and congruence endpoints
- RRx-001: binds and oxidizes hemoglobin
- Being assessed in a phase 2 IV formulation
- An oral formulation is in development
- SGX94 (dusquetide): an innate defense regulator
- Being assessed in a phase 3 IV formulation
- BMX-001: mimetic of manganese superoxide dismutase
- Being assessed in a phase 2 subcutaneous injection formulation
There are other prevention strategies such as increasing excretion with oral ingestion of vitamin C, and reducing off target binding with another antibody such as J591 (Ac225-J591), which does not reach the apical lumen. However, 225Ac as an alpha particle has more effects due to increased relative biological effect on the salivary gland. Supportive care interventions include oral moisturization with xylitol (positive effects on oral health and teeth) and coconut oil. Post-treatment interventions include sialogogues such as pilocarpine, cevimeline, and bethanechol.
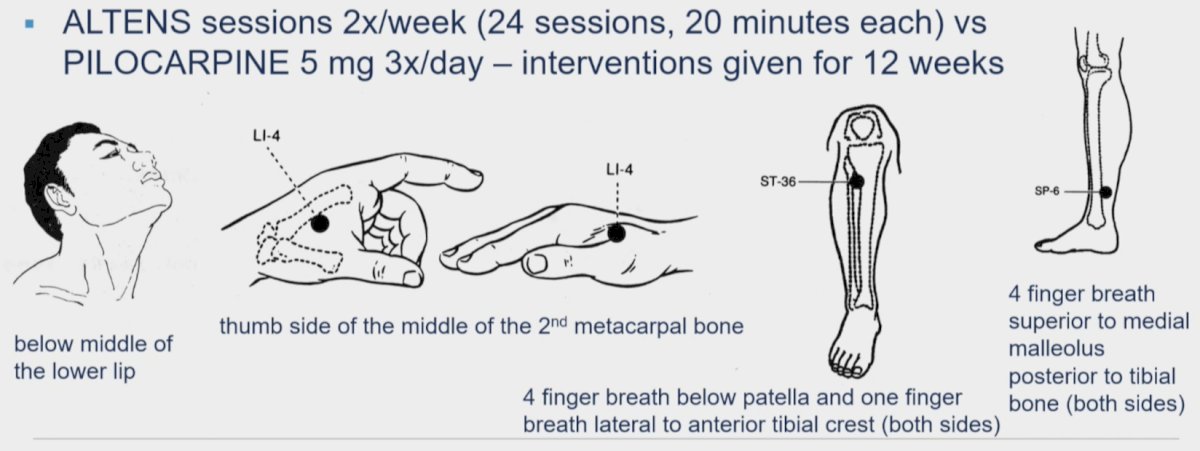
Dr. Yom’s group was part of the RTOG 0537 trial assessing acupuncture-like transcutaneous electrical nerve stimulation (ALTENS) versus pilocarpine in treating radiation-induced xerostomia.4 Eligible patients (n = 148) included those who completed head and neck radiation 3 to 24 months ago and had grade 1 xerostomia. ALTENS sessions were 2x/week (24 session, 20 minutes each) versus pilocarpine 5 mg 3x/day, with the intervention continued for 12 weeks:
The endpoint for this trial was a change in the xerostomia-related quality of life scale score over 9 months from enrolling. Changes in xerostomia-related quality of life scale scores at 9 and 15 months were -0.53/-0.27 (p = 0.45) and -0.6/-0.47 (p = 0.21). Grade 1-3 adverse events were 20.8% in the ALTENS arm and 61.6% in the pilocarpine arm. However, the machine was expensive, and many patients prefer traditional acupuncture.
Dr. Yom’s group also ran a feasibility and efficacy trial of a handheld humidification device published in 2017 [5]. In this trial of 20 patients, compliers had an average of nearly two less head and neck symptoms (-1.8, 95% CI -4 to 0.2; p = 0.08) than non-compliers at 6 weeks and fewer symptoms at 12 weeks. Generally, humidification during radiotherapy is associated with fewer head and neck symptoms among compliers and tend to have better overall head and neck-related quality of life.
Dr. Yom also addressed fluoride and calcium application for dental enamel. Among those with xerostomia, diligent oral hygiene is a must, including flossing daily, keeping the mouth hydrated, as well as 3-4 month dental exams and cleanings. Toothpaste type is important and should include 1.1% sodium fluoride, and patients should brush 2x a day for a minimum of 2 minutes or use trays/carriers for application of sodium fluoride. Patients should be counseled not to eat, drink, or rinse for 30 minutes after brushing their teeth with sodium fluoride toothpaste. Other options for oral hygiene include baking soda rinses, which provide somewhat similar effects. Dental health is also very important to patients, highlighted by the following quote from a patient advocate “the prospect of the loss of one’s teeth is terrifying to comprehend. Impossibly so…encourage patients to use their dental trays in the shower. It gives them a regular routine to use them and they are able to spit excess fluoride saliva down the drain.” Supplementation of 1.1% fluoride gel during and after radiotherapy also decreases dental caries during radiation. Strict and regular usage is most important: the risk of cavities among compliant patients at 12-36 months using daily gel in a carrier or twice daily tooth brushing is essentially zero. One new technology being investigated is the gene therapy-based transfer of aquaporin complement DNA into salivary glands:

Finally, Dr. Yom addressed stem cell regenerative therapy, which is being evaluated in the marrow-derived autologous stromal cells for the restoration of salivary hypofunction (MARSH) study. This is a phase 1 dose-escalation trial of patients with xerostomia after radiation therapy for head and neck cancer.
Dr. Yom concluded her presentation discussing the management of dry mouth with the following take-home points:
- It is important to have a longitudinal clinic presence:
- Preventative: blockade, radioprotection, increased excretion (vitamin C), reducing off-target binding
- Supportive: moisturization (rinses, sialogogues), acupuncture, humidification, dental care, reversal therapies
- Emotional/psychological support, counseling, and reinforcement is important
- Management of referrals and coordination with dental, nursing, swallowing, and oral medicine support services is crucial
Presented by: Sue Yom, MD, PhD, University of California, San Francisco, San Francisco, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Pepin A, Kiess A, Lukens JN, et al. Management of dry mouth toxicity following 177Lu-PSMA-617 radioligand therapy. Pract Radiat Oncol. 2025 Jan-Feb;15(1):14-18.
- Sathekge MM, Lawal IO, Bal C, et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): A multicentre, retrospective study. Lancet Oncol. 2024 Feb;25(2):175-183.
- Wong RKW, Deshmukh S, Wyatt G, et al. Acupuncture-like transcutaneous electrical nerve stimulation versus pilocarpine in treating radiation-induced xerostomia: Results of RTOG 0537 phase 3 study. Int J Radiat Oncol Biol Phys. 2015 Jun 1;92(2):220-227.
- Ghosh P, Lazar AA, Ryan WR, et al. A feasibility and efficacy trial of a hand-held humidification device in patients undergoing radiotherapy for head and neck cancer. Support Care Cancer. 2017 Aug;25(8):2611-2618.