(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a LuPSMA therapy session and a presentation by Dr. Luke Nordquist discussing PSMA radioligand therapy in a medical oncology private center. Community oncology centers play an important role, as more than 50% of cancer patients in the United States receive their care at community cancer centers. The benefits of a community oncology center are that it (i) expands access to innovative treatments for patients closer to home, and (ii) maintains established local support and patient-provider relationships. However, there are certain struggles:
- These centers often lack the experience, resources, or reputation to establish a research program
- These centers are often facing significant financial strains limiting their ability to develop new programs, research, or theranostic programs
Notably, there are high costs to develop a community “medical oncology” theranostic program. The following shows 2025 data from four medical oncology practices in Dothan, AL:
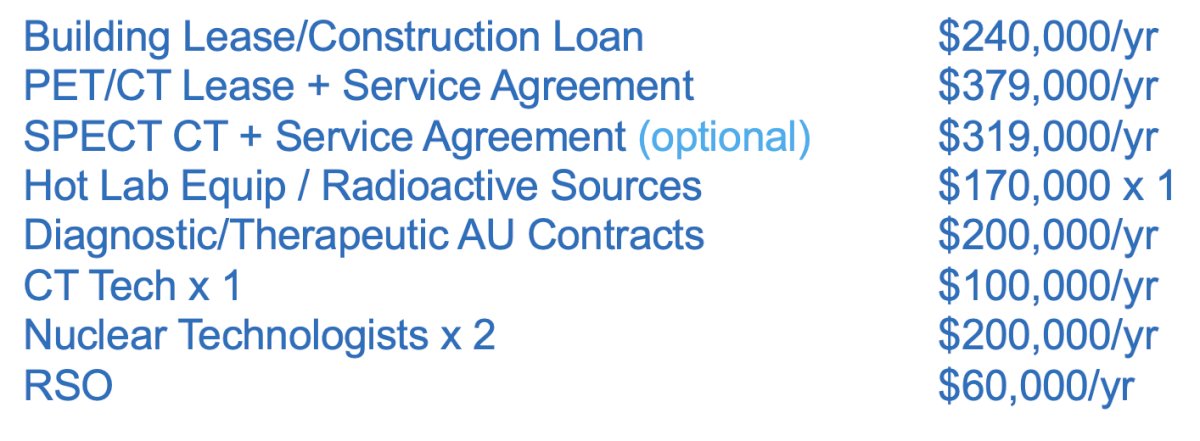
Taken together, this includes a $1.4-1.7 million cost in year 1 and annual costs of $1.2-1.5 million in annual costs. New challenges and unchartered waters include the following considerations:
- Regulatory and licensing hurdles: RAM licensing and radiation safety compliance
- New infrastructure: hot lab, uptake rooms, storage/waste, radiation monitoring, and split protocols
- Expanding staffing: nuclear techs, CT techs, RSO, and authorized user contracts
- New collaborations: radiopharmacies, couriers, and waste disposal
- Complete scheduling and workflow: handling isotope half-life timing, coordinating patient visits, as well as radiotracer preparation and administration
- Reimbursement complexities: separate reimbursement for drug, imaging, and administration
So, is this worth all of the cost and effort for two FDA approved therapies (177Lu-PSMA-617 and 177Lu-dotatate)? Dr. Nordquist suggests that clinical trial participation is a potential solution noting that (i) it is a new and significant source of revenue for the clinic, (ii) it provides innovative therapies for patients that are closer to home (more hope), (iii) lower financial toxicity for patients, (iv) marketable differences for competitors and a reputation for excellence, (v) physician and staff professional development, and (vi) an opportunity to be a part of new science.
Dr. Nordquist states that XCancer was founded in 2010 to conduct innovative prostate cancer clinical trials in a high quality and efficient manner, and to expand the reach of these trials to other community cancer centers. There are 50+ staff with a focus on clinical trials, 100% of patients are evaluated for a clinical trial, with nearly 2,000 patients enrolled on trials to date, including 23 first-in-world trials. Study feasibility to patient accrual time is typically only 2-8 weeks led by proprietary research software for quality and efficiency. There is also central RECIST radiology available. More than 40 community cancer centers have utilized the XCancer program, staff, training, software, and ongoing support and processes.
Regarding the XCancer theranostic trials model, this includes 50+ phase 0-3 trials, including the first 17 patients enrolled in the VISION1 trial. Moreover, five XCancer theranostic trial sites accrued patients on the VISION trial, leading Novartis to state “XCancer has the highest quality data of all participating sites.” Isotopes being assessed in XCancer theranostic trials includes: Ga68, F18, Cu64, Zr89, Tc99, In111, Ra223, Lu177, Cu67, Ac225, Th227, and Pb212. XCancer has five nuclear techs and 14 AUs on contract, has PET/CT and SPECT CT capabilities, as well as a gamma camera. Other consultation services available include RSO, AU, and health physics.
There are several reasons to develop theranostic clinical trial sites in the community:
- It is estimated that 50% of oncology clinical trials close due to poor accrual
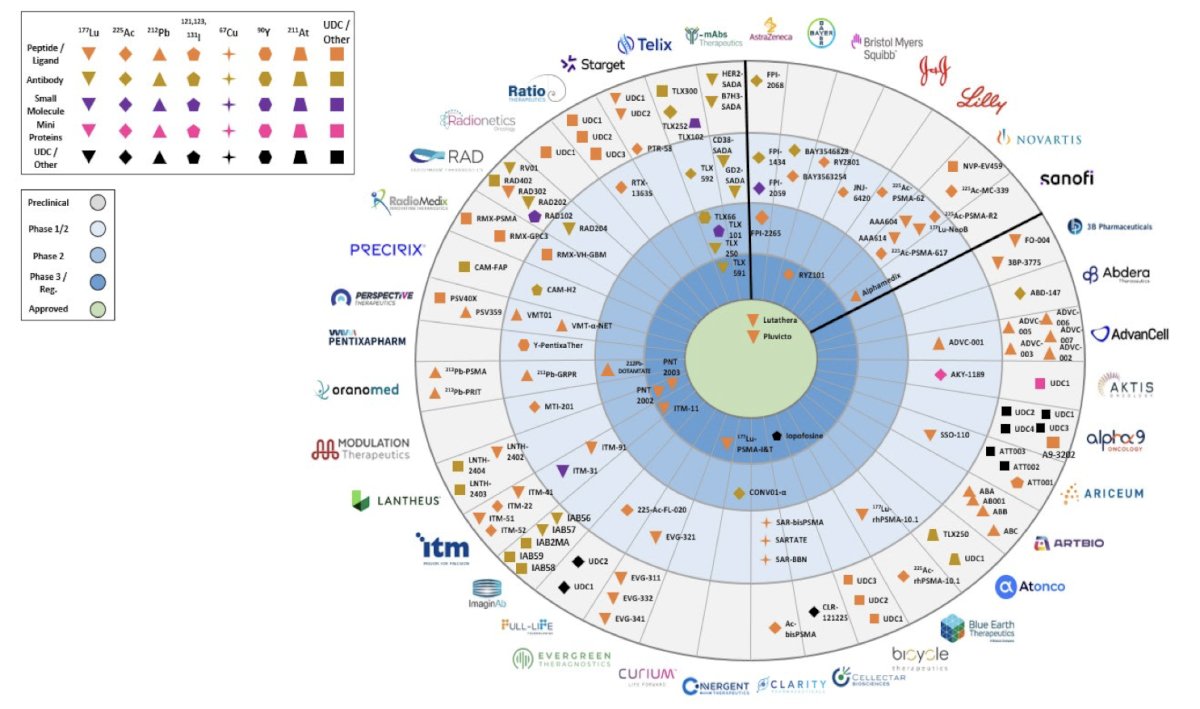
- There has been rapid growth of theranostic clinical trials (nearly 700 today)
- This brings the “real world experience” to clinical trials
- The sleeping giant: more than 50% of metastatic cancers are treated at community cancer centers
Globally, there has been a rapid growth of theranostic clinical trials: from 155 trials in 12 cancer subtypes in 2022 to 670 trials in 35 cancer subtypes in 2025:
Dr. Nordquist then discussed theranostictrials.org, a website for tracking theranostic trials that he and his team has developed:
To date, there are 671 theranostic trials listed on the website, with detailed information including the sponsor and the trial principal investigator.
Dr. Nordquist concluded his presentation by discussing PSMA radioligand therapy in a medical oncology private center with the following take home points:
- Bringing theranostics into the community setting would dramatically expand the access for more cancer patients, but there are major challenges
- Success requires thoughtful strategy, investment, infrastructure, education, personnel, licensing, and collaboration
- A well developed and focused theranostic clinical trials program is one solution
Presented by: Luke Nordquist, MD, Xcancer, Omaha, NE
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References: