(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a PSMA session and a presentation by Dr. Michael Morris discussing incorporating PSMA PET into clinical trials. There are many challenges with regard to upstaging, downstaging, and different detection rates of existing and new lesions when moving from conventional imaging to PSMA PET:1
PSMA has variable expression in mHSPC, in particular relative to mCRPC, similar to a flare phenomenon on bone scans. Currently, there are many reporting recommendations: PrimaryScore, PROMISE, ePROMISE, aPROMISE, PSMA-RADS, ePSMA, PPP (PSMA PET Progression criteria), RECIP, PCWG3 (PWG4), RECIST 1.1, and aPERCIST. The 30 experts in SPARC include:

These experts were split into 5 thematic groups and each group reviewed relevant literature to generate agreement statements. Then, a preview and refinement process of all statements was completed by all 3 experts on the panel, with 91 final statements created.
There are several clinical trial considerations noted by Dr. Morris:
- Right now we are still “stuck” with bone scans as a standard for clinical trials – PSMA PET should be performed in studies at baseline, early response, and early progression
- Overall:
- Clinical trials are international, involving sites of various resources and sophistication
- Criteria need to be feasible on standard workstations
- Cannot involve proprietary software that only certain sites have
- Response: currently we cannot define an investigational endpoint. Data collection is needed so that we have answers for PCWG5
- Progression:
- SUV based criteria require validation
- New lesions do represent progressive disease
Dr. Morris notes that there are several common assumptions shared between SPARC and PCWG4:
- No validated response/progression criteria for SUV based changes
- RECIST will still apply despite PSMA PET
- There are no absolute cutoffs: new lesions will be defined on the basis of uptake, size, location, and pattern rather than a simple SUV-based cutoff
- Early PSMA imaging can reflect changes in PSMA uptake rather than response or progression of disease
With regards to eligibility, for standard imaging, this will be the same as for PCWG3. For appropriate trials, for PSMA PET, changes in SUV based criteria are not ready to qualify as progression of disease, whereas new lesions will qualify if a prior PSMA PET is available for comparison. The response criteria are to collect PSMA PET data in addition to standard imaging algorithms.

Dr. Morris notes that what we know is that new metastatic disease is, at face value, bad. Metastasis free survival is not a surrogate or intermediate endpoint, it is, itself, a clinically relevant endpoint. In work from Dr. Morris’ group2 assessing PCWG3, they noted that more disease over threshold does not confer a greater association between radiographic progression free survival and overall survival:

For progression with PSMA PET, (i) it is important to distinguish oligometastatic from polymetastatic progression of disease, (ii) when imaged with PSMA PET, polymetastatic progression of disease will not require a confirmatory scan, and (iii) some visceral lesions, even if only evident on PET, are worthy of declaring progression of disease.
Dr. Morris concluded his presentation by discussing incorporating PSMA PET into clinical trials with the following take home points:
- PSMA PET will likely augment, rather than replace, conventional imaging for now
- PSMA PET metastasis free survival may not require further regulatory qualification, but further discussion is needed
- PSMA PET response is not yet ready for prime time
- PSMA PET radiographic progression free survival (and conventional radiographic progression free survival) can be made safe without likely losing an association with overall survival
Presented by: Michael Morris, MD, Memorial Sloan Kettering, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
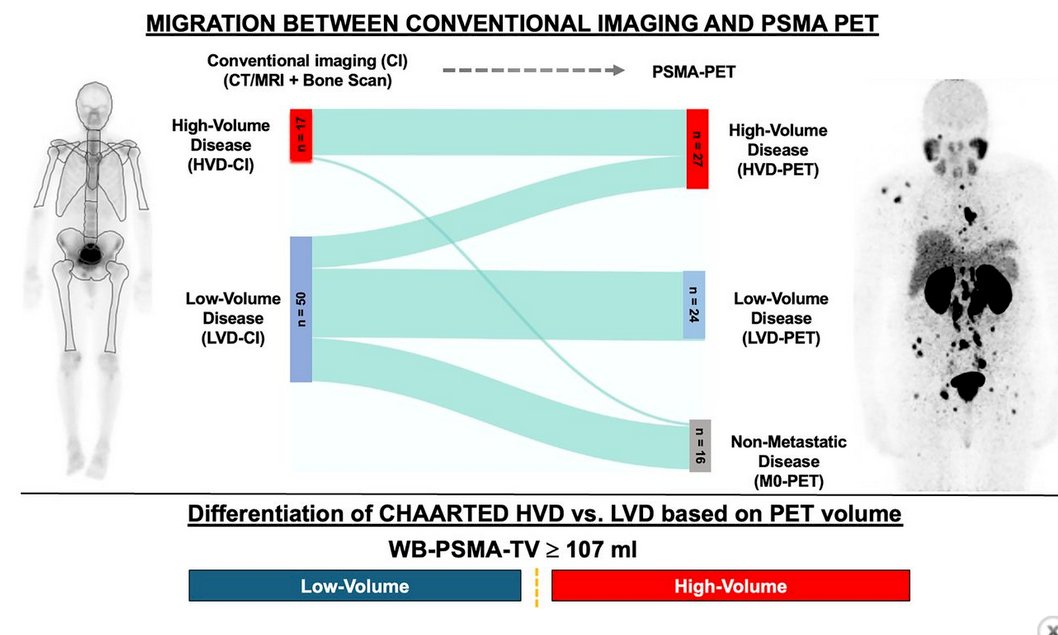
- Unterrainer LM, Hope TA, Fendler WP, et al. Low- and high-volume disease in metastatic hormone-sensitive prostate cancer: From CHAARTED to PSMA-PET—An International Multicenter Retrospective Study. J Nucl Med. 2025 Jan 3;66(1):54-60.
- Anand A, Heller G, Fox J, et al. Automated bone scan index to optimize Prostate Cancer Working Group radiographic progression criteria for men with metastatic castration-resistant prostate cancer. Clin Genitourin Cancer. 2022 Jun;20(3):270-277.