(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a PSMA session and a presentation by Dr. Emmanuel Antonarakis discussing the impact of clinical guidelines on the utilization of PSMA PET. For this presentation, Dr. Antonarakis discussed the NCCN guidelines (v1.2025), SNMMI Appropriate Use Criteria (2023), and AUA/SUO Guidelines (2023). The NCCN guidelines recommend the currently FDA-approved PSMA agents, F-18 piflufolastat (DCFPyL), F-18 flotufolastat, and Ga-68 PSMA-11. NCCN also notes that PSMA PET imaging has a higher sensitivity than C-11 choline or F-18 fluciclovine PET imaging. The panel also believes that both Ga-68 PMSA-11, F-18 flotufolastat, or F-18 piflufolastat PSMA imaging can be used to determine eligibility of patients for Lu-177 PSMA-617 therapy. There are several indications for PSMA PET imaging according to the NCCN guidelines:
- Initial risk stratification for localized prostate cancer for patients at unfavorable intermediate, high, or very high risk
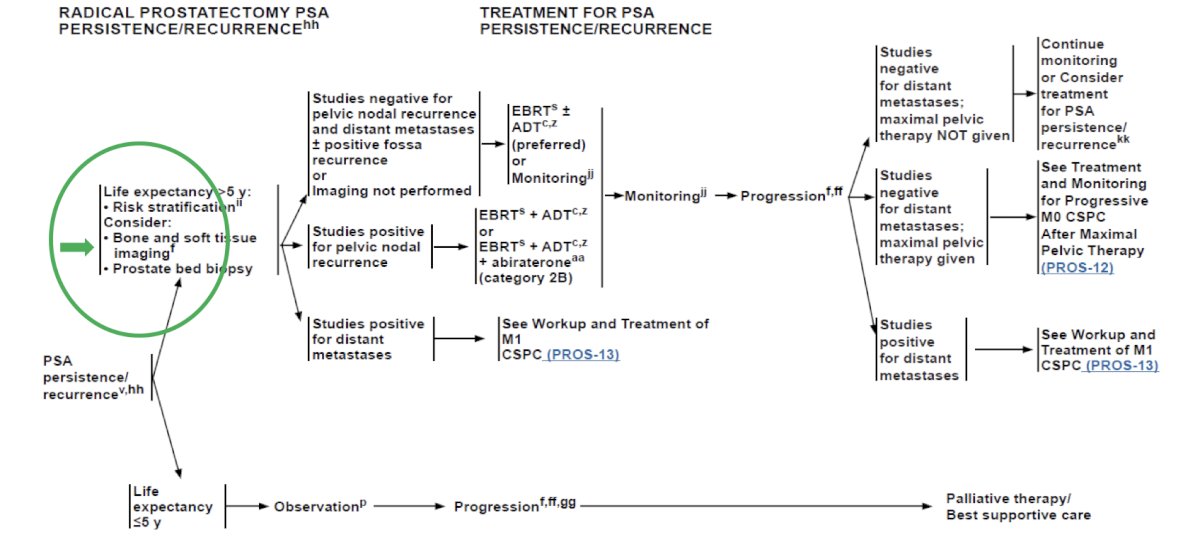
- Detection of biochemical recurrent disease after radical prostatectomy
- Detection of biochemical recurrent disease after radiation therapy
- Workup for progression
Because of the increased sensitivity and specificity of PSMA-PET tracers for detecting micrometastatic disease compared with conventional imaging (CT, MRI) at both initial staging and biochemical recurrence, the NCCN panel does not feel that conventional imaging is a necessary prerequisite to PSMA-PET and that PSMA PET/CT or PSMA PET/MRI can serve as equally effective, if not more effective, front line imaging tools for these patients. Appropriate staging imaging is particularly important for correctly assessing disease burden and subsequently treating high or very high risk patients:
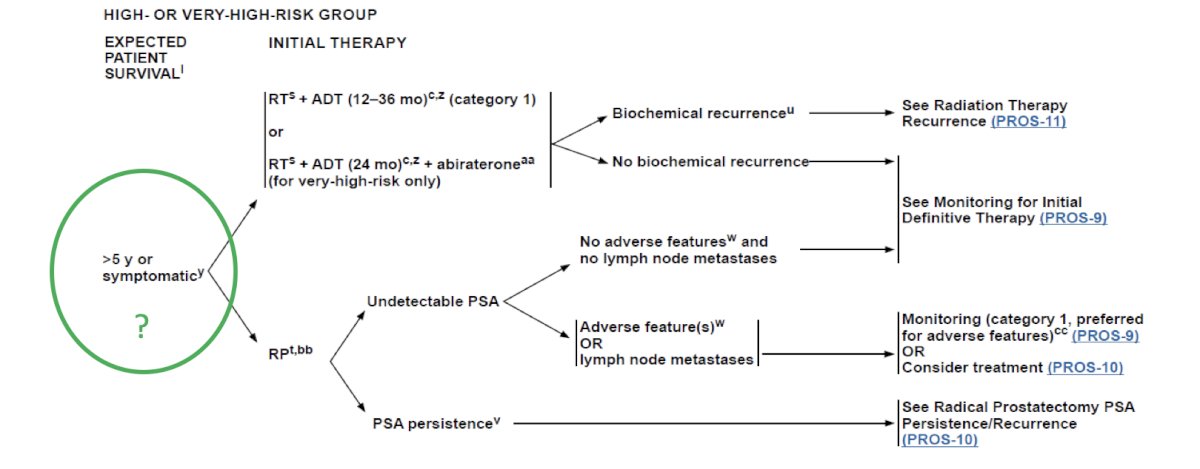
Moreover, appropriate staging of patients after radical prostatectomy with PSA recurrence or persistence has downstream treatment implications:
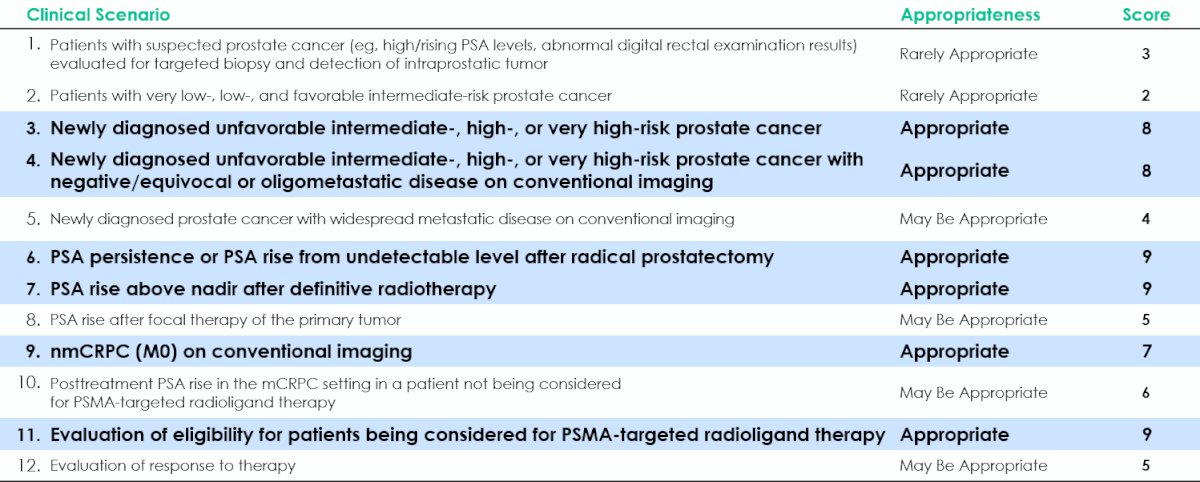
Dr. Antonarakis also emphasized that PSMA PET SUVmean is predictive for Lu-177-PSMA-617 therapy. The SNMMI Appropriate Use Criteria is a very helpful delineation of different case situations where PSMA PET may or may not be useful:1
The AUA/SUO guidelines for biochemical recurrence without metastatic disease after exhaustion of local treatment options suggest the following:2
- Both 68Ga-PSMA-11 and 18F-DCFPyL are indicated for patients with suspected prostate cancer metastasis considering local therapy, as well as for patients with suspected prostate cancer recurrence based on elevated PSA levels (Clinical Principle)
- Clinicians should utilize PSMA PET imaging preferentially, where available, in patients with PSA recurrence after failure of local therapy as an alternative to conventional imaging due to its greater sensitivity, or in the setting of negative conventional imaging (Expert Opinion)
- PSMA PET availability is increasing in the US and detects metastatic disease at low PSA values
The AUA/SUO guidelines for nonmetastatic castration-resistant prostate cancer (nmCRPC) suggest the following:2
- Clinicians should assess nmCRPC patients for development of metastatic disease using conventional or PSMA targeted PET imaging at intervals of 6 to 12 months (Expert Opinion)
- The suggested interval for imaging is 6-12 months, with the exact interval determined by the PSA doubling time calculation, the development of symptoms, and patient/physician preference
For mCRPC, the AUA/SUO guidelines state clinicians should offer 177Lu-PSMA-617 to patients with progressive mCRPC having previously received docetaxel and androgen receptor pathway inhibitor with a positive PSMA PET study (Strong Recommendation: Evidence Level Grade B). Finally, for metastasis directed therapy, the guideline notes:
- Given the ability to identify metastatic sites earlier than was previously possible using newer PET imaging modalities, there has been renewed interest in the concept of metastasis directed therapy with radiation, surgery, or ablative technologies
- ORIOLE3 had 54 patients that were randomized to receive stereotactic ablative radiotherapy or observation alone using PSMA PET imaging – consolidation of all PSMA positive disease decreased the risk of new lesions at 6 months (16% versus 63%, p = 0.006)
Dr. Antonarakis concluded his presentation by discussing the impact of clinical guidelines on the utilization of PSMA PET by emphasizing areas not covered by the NCCN, SNMMI, and AUA guidelines:
- Using PSMA PET to quantify tumor burden
- Using PSMA PET to determine radiographic progression free survival
- Using PSMA PET for assessing disease response
- PCWG4: how to use PSMA PET in clinical trial design framework with focus on drug/biomarker development
- SPARC: how PSMA PET should be reported, used for staging, biochemical recurrence detection, and response assessment
Presented by: Emmanuel Antonarakis, University of Minnesota, Minneapolis, MN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Jadvar H, Calais J, Fanti S, et al. Appropriate Use Criteria for Prostate-Specific Membrane Antigen PET Imaging. J Nucl Med. 2022 Jan;63(1):59-68.
- Lowrance W, Dreicer R, Jarrad D, et al. Updates to Advanced Prostate Cancer: AUA/SUO Guideline (2023). J Urol. 2023 Jun;209(6):1082-1090.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.