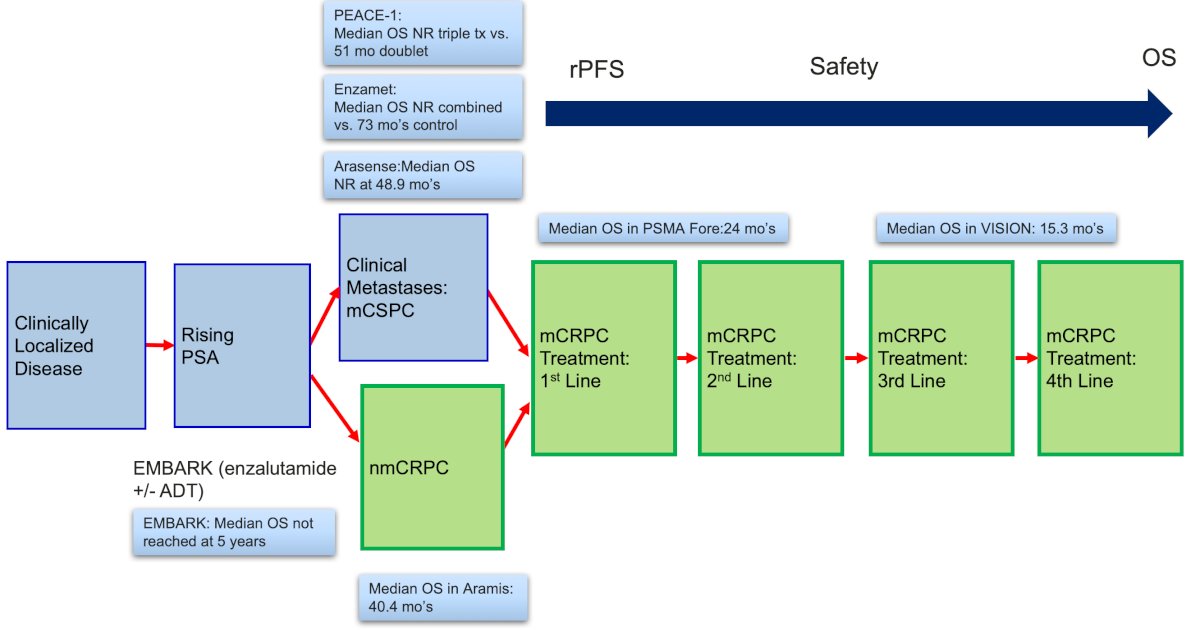
(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a LuPSMA therapy session and a presentation by Dr. Michael Morris discussing moving into the castration sensitive setting. Dr. Morris notes that treating early has some unique design issues as highlighted in the following figure:
Dr. Morris then discussed the PSMAddition trial which is assessing 177Lu-PSMA-617 + standard of care versus standard of care in mHSPC in a phase 3 randomized clinical trial. The primary endpoint is radiographic progression free survival:
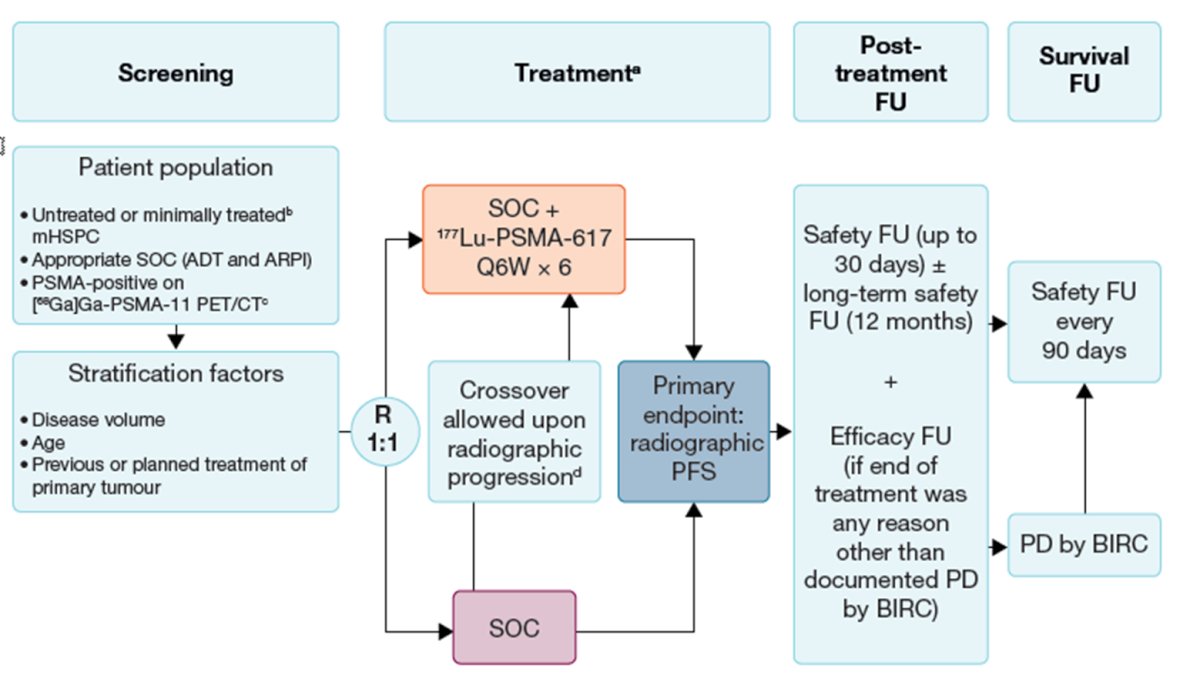
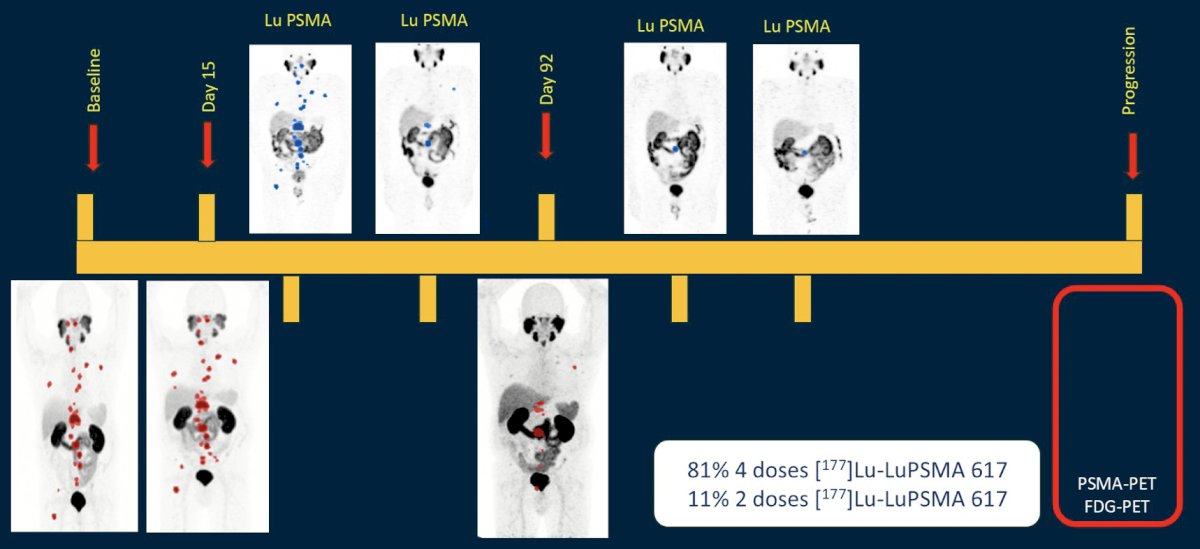
Patients in the 177Lu-PSMA-617 arm will receive six upfront cycles of therapy and then continue on with ADT + androgen receptor pathway inhibitor. Patients in the control arm that experience radiographic progression are allowed to cross over to 177Lu-PSMA-617 therapy. Dr. Morris notes that the ENZA-p trial, with updated results presented at ASCO GU 2025, utilized adaptive dosing, with 81% of patients in this trial undergoing 4 doses of 177Lu-PSMA-617 and 11% undergoing 2 doses of 177Lu-PSMA-617:
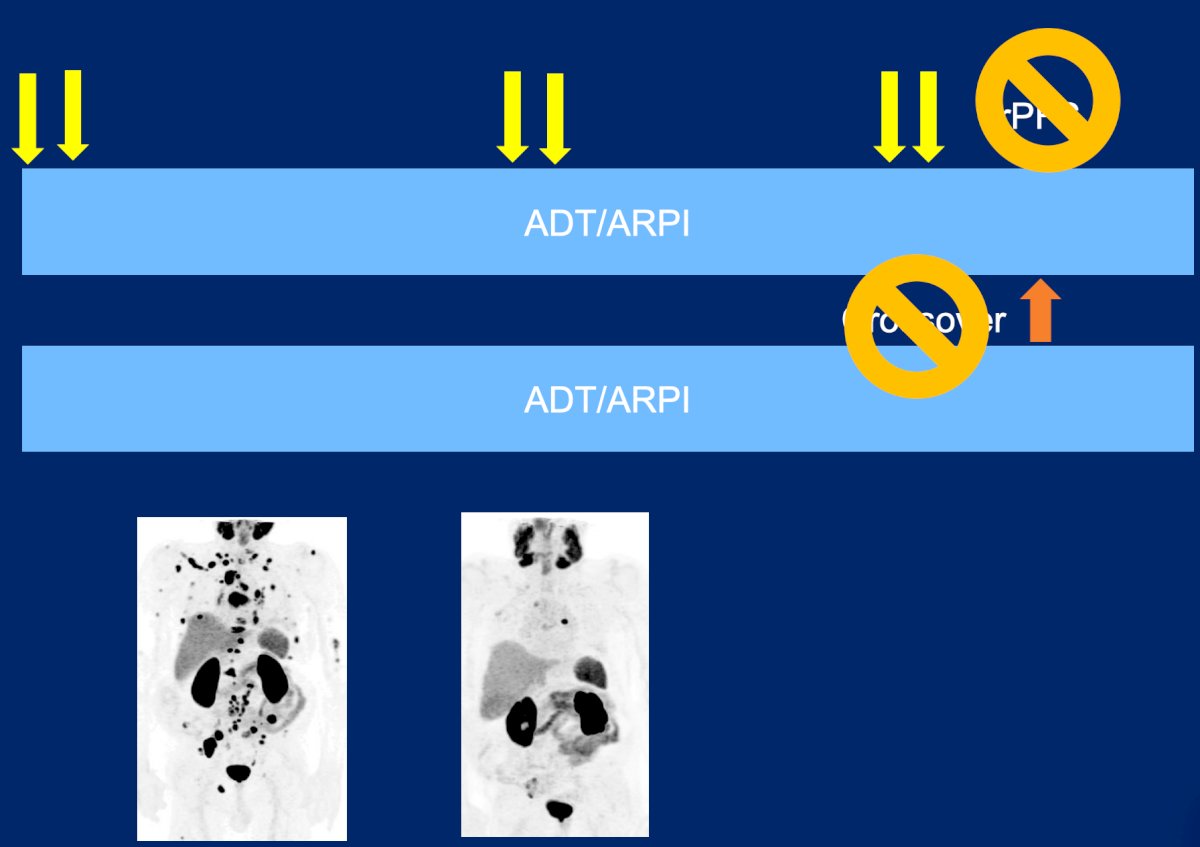
He argues that in PSMAddition, crossover should be standard of care use of radioligand therapy downstream, and to subsequently power the study for overall survival:
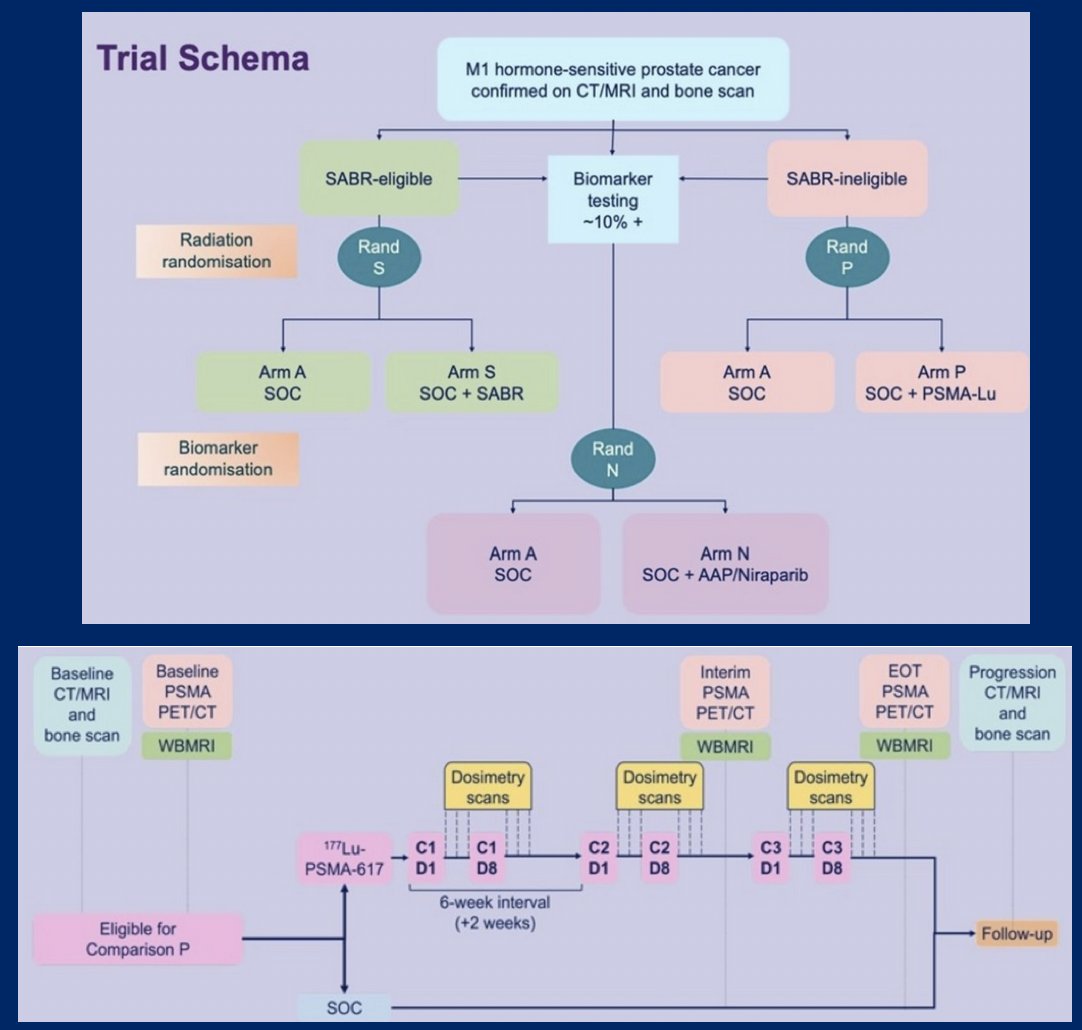
Next, Dr. Morris discussed the STAMPEDE2 trial, which is assessing 177Lu-PSMA-617 at 7.4 GBq on day 1 and day 8, with 3x6 weekly cycles. The primary outcome is radiographic progression free survival and overall survival, with secondary outcomes including failure free survival, prostate cancer specific survival, safety, toxicity, compliance, cost, and resources. The complete trial design is as follows:
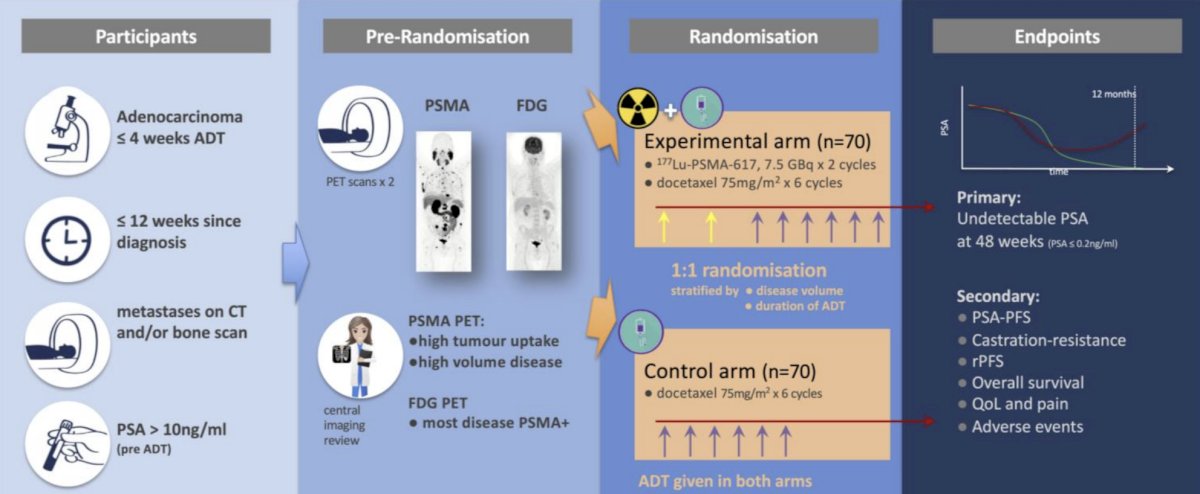
The UpFrontPSMA trial1 was published in 2024 and included patients with de novo high-volume mHSPC who had received ≤4 weeks of ADT and had a PSA >10 ng/ml at diagnosis. Prior to randomization patients underwent both PSMA and FDG PET scans. Eligibility was limited to those patients with evidence of high tumor uptake and high-volume disease on PET scans. Patients were also required to have the majority of their metastatic disease demonstrating PSMA positivity. Eligible patients were randomized to:
- Experimental arm: 177Lu-PSMA-617 7.5 GBq x 2 cycles + docetaxel 75 mg/m2 x 6 cycles
- Control arm: Docetaxel 75 mg/m2 x 6 cycles
Between May 2020 and April 2023, 130 patients were recruited and underwent randomization (experimental: 63, control: 67). All 63 patients in the experimental arm completed the two cycles of 177Lu-PSMA-617, and 79% of patients in the combination arm completed all 6 cycles of docetaxel, compared to 84% of patients in the control arm. However, a docetaxel dose reduction was required in 33% of patients in the combination arm, compared to 17% of patients in the docetaxel arm.
For the primary outcome, an undetectable PSA at week 48 was observed in 41% of patients in the 177Lu-PSMA-617 + docetaxel arm versus 16% of patients in the docetaxel control arm (OR 3.88, 95% CI 1.61–9.38, p = 0.002). An undetectable PSA at any point was observed in 51% and 32% of patients, respectively (OR 2.14, p = 0.042). Time-to-event analyses demonstrated that patients in the experimental arm had superior PSA progression-free survival (median: 31 versus 20 months; HR 0.60, p = 0.039):

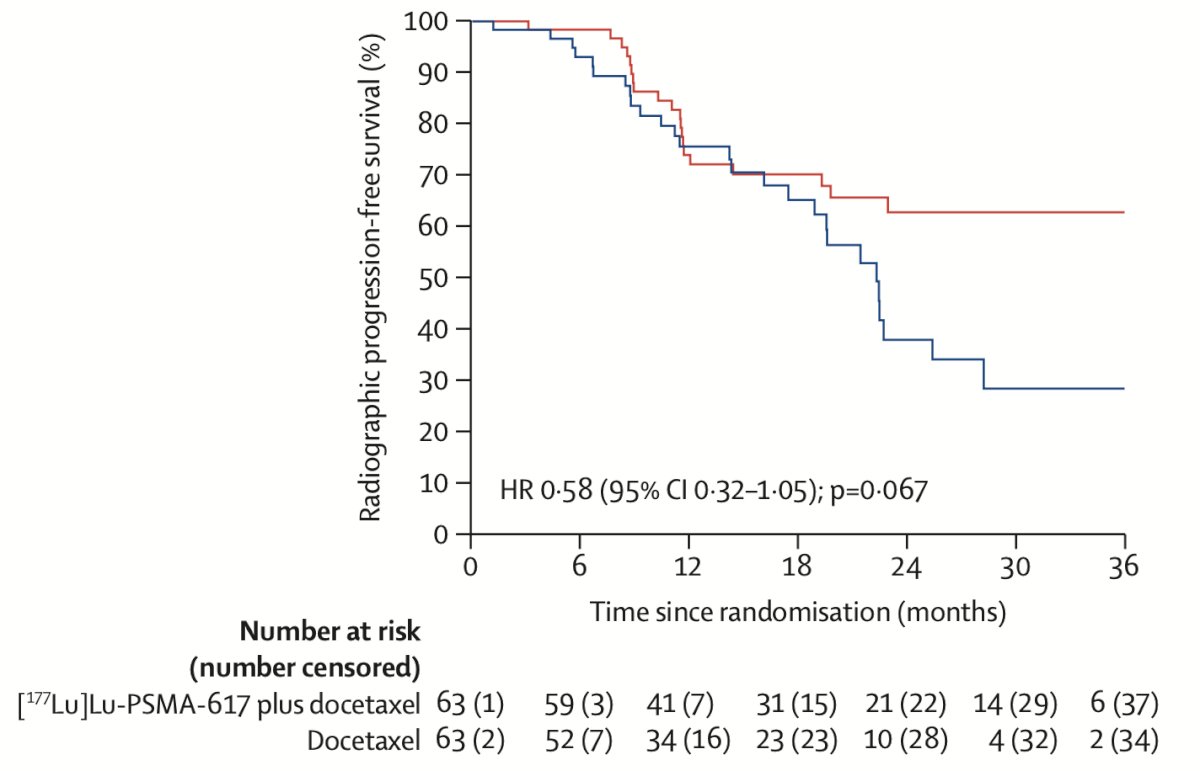
Radiographic progression-free survival similarly favored 177Lu-PSMA-617 + docetaxel (HR 0.58, p = 0.067):
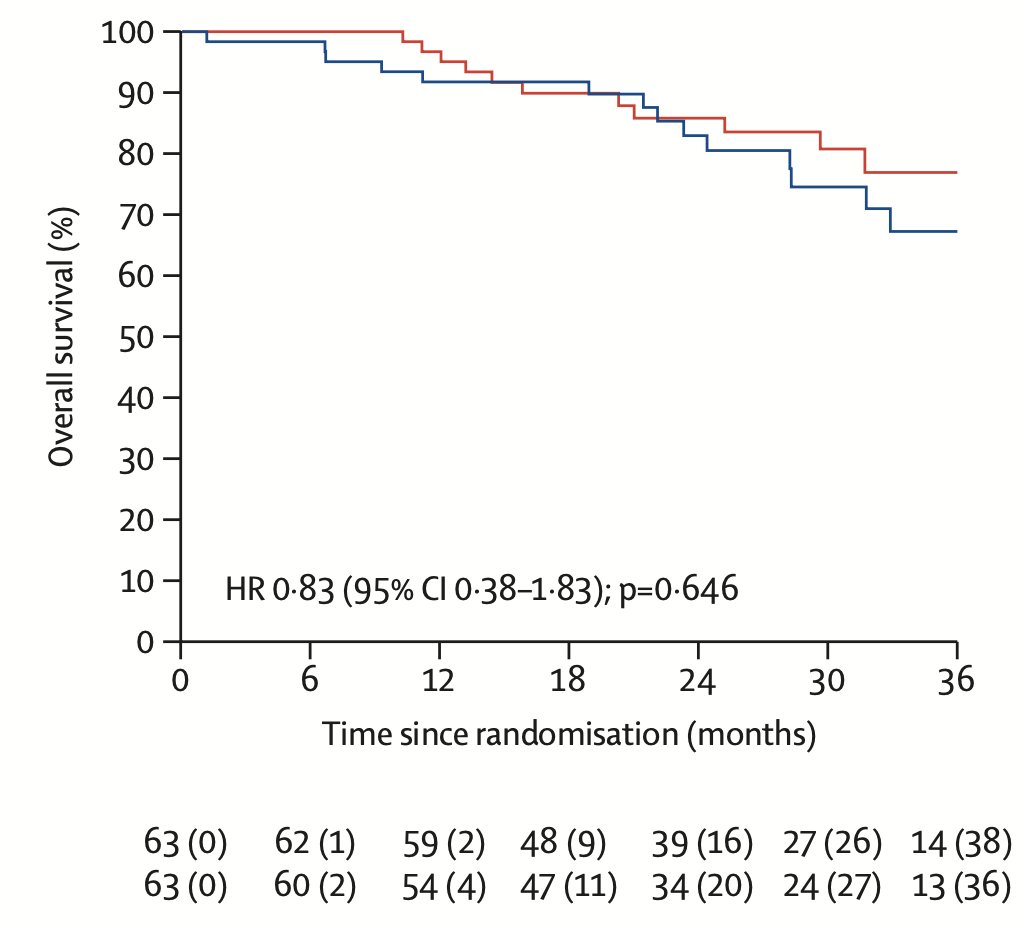
To date, there is no overall survival benefit with the addition of 177Lu-PSMA-617 to docetaxel (HR 0.83, 95% CI: 0.38–1.83, p = 0.646):
Dr. Morris concluded his presentation by discussing moving into the castration sensitive setting with the following take home points:
- Timelines are long, and so concerns about longer term toxicity come into play, including the bone marrow, kidneys, and secondary malignancies
- This is the space to consider alternative dosing schedules to optimize the distinguishing properties of radioligand therapy from other systemic therapies, such as adaptive dosing and upfront intensification
- Implications of this approach can impact endpoints, such as radiographic progression free survival and overall survival
- There may eventually be consideration of intensification strategies versus finally approaching a point of testing replacement for ADT, even in polymetastatic disease
Presented by: Michael Morris, MD, Memorial Sloan Kettering, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Azad AA, Bressel M, Tan H, et al. Sequential [(177)Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone sensitive prostate cancer (UpFrontPSMA): A multicentre, open label, randomized, phase 2 study. Lancet Oncol. 2024 Oct;25(10):1267-1276.