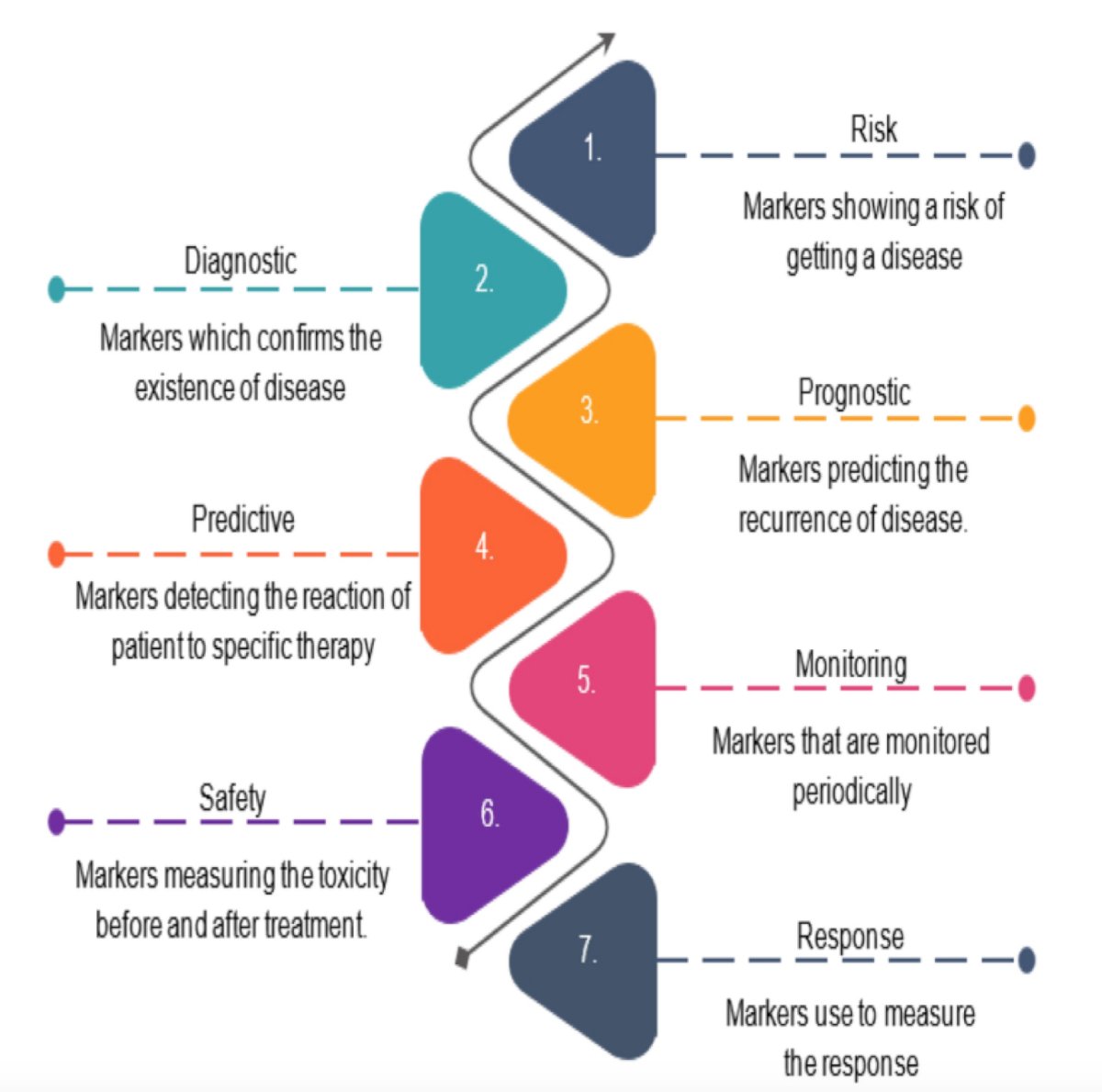
(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a PSMA session and a presentation by Dr. Daniel Spratt discussing whether we can kill the bone scan. There are several roles for diagnostic tests in medicine as highlighted in the following figure:
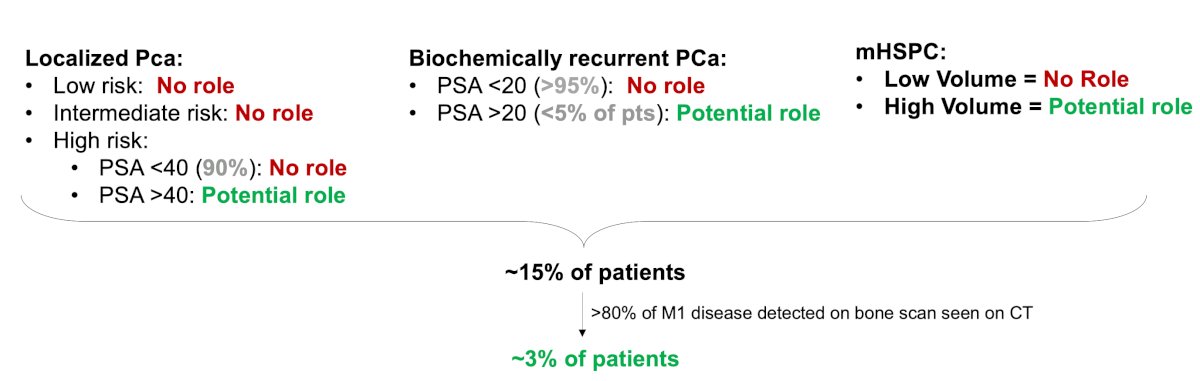
Stated another way, the simplistic goal of cancer imaging is to detect cancer. The goal of cancer imaging is not itself to improve quality or quantity of life, which is the goal of a therapeutic intervention. So, if the goal of cancer imaging is to detect cancer, what is the role of a bone scan? Dr. Spratt notes that there is no role in T-staging, N-staging, M1a (distant lymph nodes), or M1c (spread to distant organs). The only role of a bone scan is for M1b (spread to the bones) staging. Bone scan may have a role in the role in the following prostate cancer disease spaces:

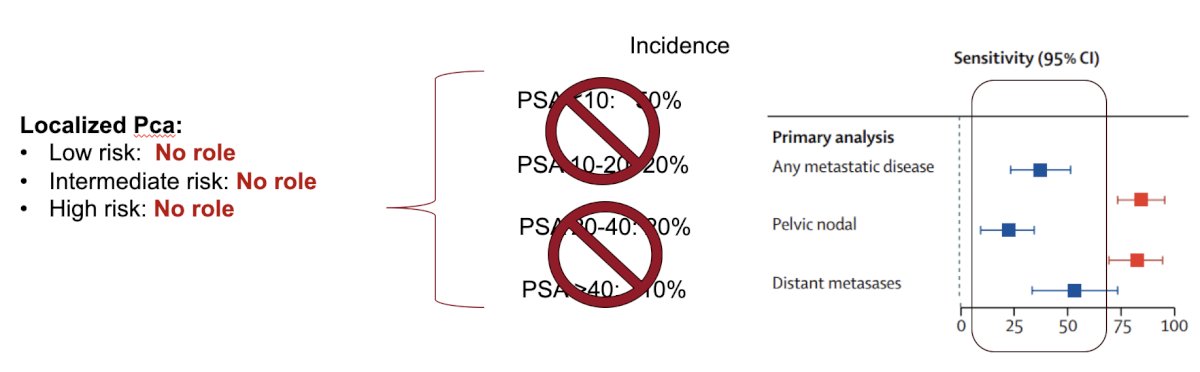
For patients with high risk localized prostate cancer, Dr. Spratt notes that the sensitivity for skeletal bone metastases compared to PSMA PET CT for a PSA < 20 ng/mL is only 46% [1]:

For a PSA > 20 ng/mL, the sensitivity for detecting skeletal metastases compared to PSMA PET/CT increases to 89%. However, when we include T3, N+, M1a, and/or M1c disease (which bone scan cannot detect), the overall sensitivity of a bone scan with a PSA > 20 ng/mL in high risk localized prostate cancer is only ~50%. In the proPSMA trial [2], conventional imaging was far less sensitive compared to PSMA PET/CT, with a sensitivity of < 50%:
Dr. Spratt emphasized that bone scan has poor performance to detect cancer in localized prostate cancer, thus it fails to meet its purpose.
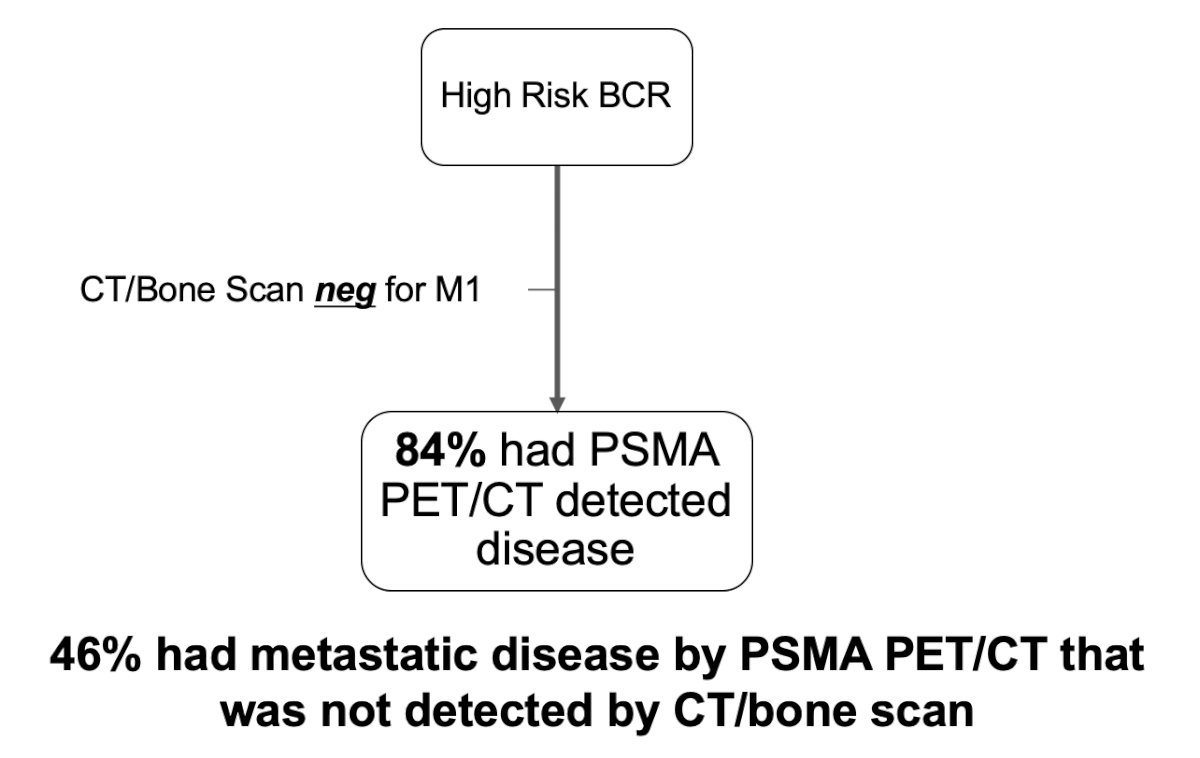
In the biochemical recurrence setting perhaps there is a potential role for bone scan among the <5% of patients with a PSA > 20 ng/mL. In the United States Veterans Affairs hospitals, 1 in 5 men who receive surgery receive a post-operative bone scan at a median PSA of 0.2 ng/mL. Moreover, in a 1998 study, the probability of a positive bone scan was < 5% until the PSA increased to 40 ng/mL [3]. This was corroborated in a 2004 study [4] that showed a bone scan in patients with PSA < 7 ng/mL is unlikely to be positive, whereas a PSA of > 20 ng/mL is more likely to be positive. In a recent study from Holzgreve et al. [5], they assessed 182 patients to describe the staging information obtained by PSMA PET/CT in a patient cohort eligible for the EMBARK trial. Results of PSMA PET were positive in 80% of patients after radical prostatectomy, 92% of patients after definitive radiotherapy, 85% of patients after radical prostatectomy and salvage radiotherapy, and 84% of patients overall. Finally, 46% of patients had metastatic disease detected on PSMA PET/CT that was not detected by CT/bone scan:
Dr. Spratt emphasized that bone scan has poor performance to detect cancer in biochemically recurrent prostate cancer, thus it fails to meet its purpose.
In the mHSPC disease space, PSMA PET/CT upstages ~40% of patients:
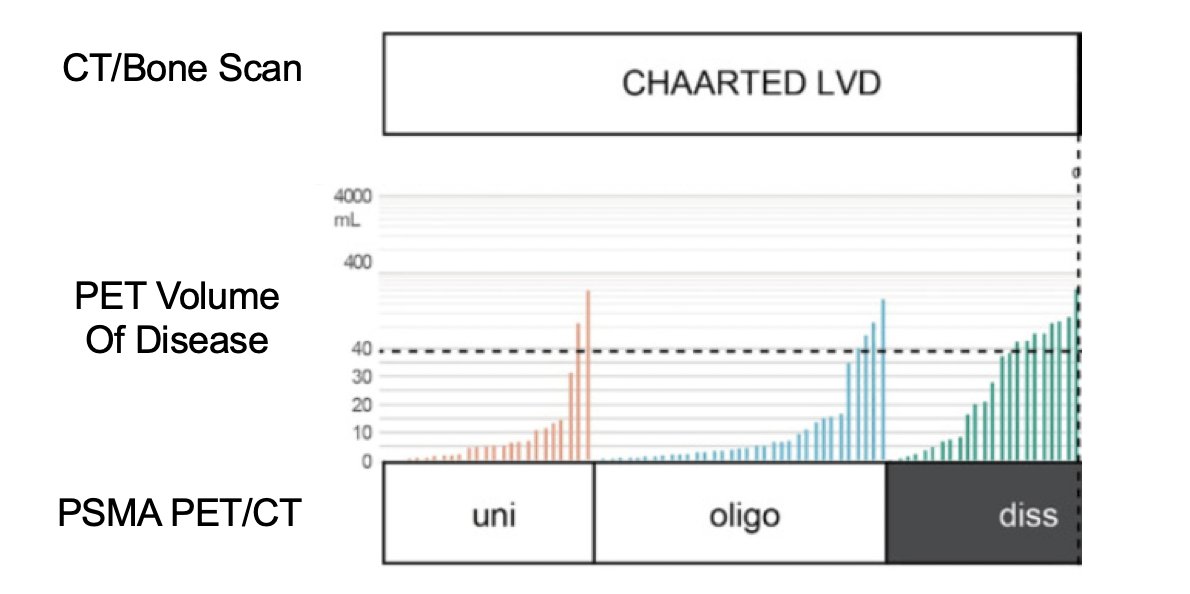
Dr. Spratt emphasized that bone scan has poor performance to detect cancer in mHSPC, thus it fails to meet its purpose. Taken together, bone scans largely fail to meet the goal of detecting prostate cancer, with only ~3% of patients potentially being appropriate for bone scan:
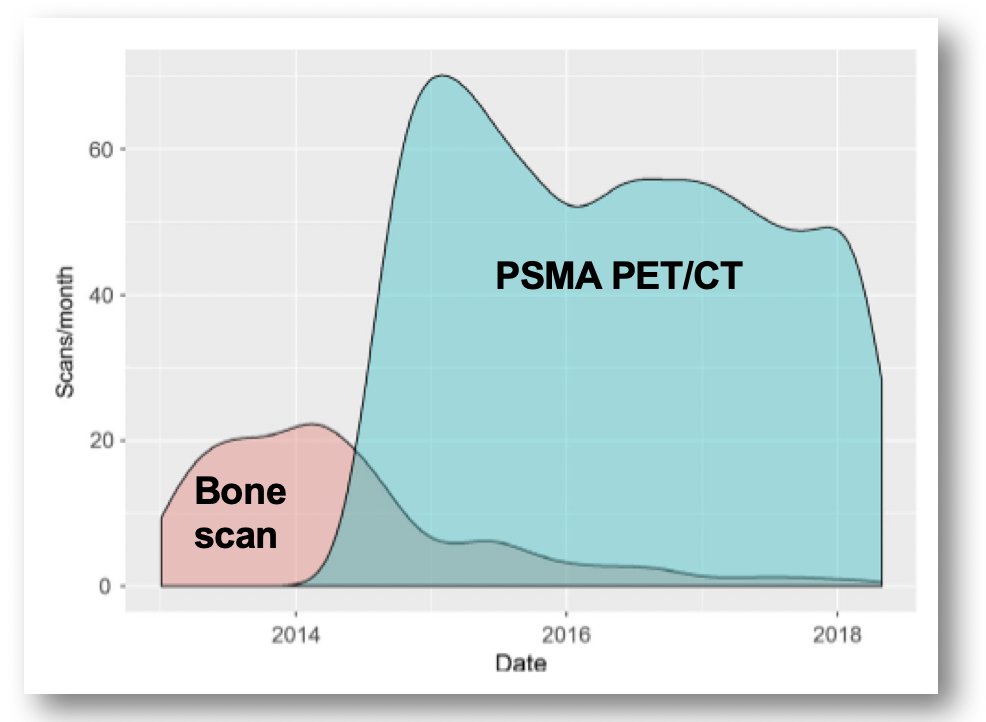
Among these 3% of patients, is a bone scan even predictive of treatment benefit? Is PSA, grade, T-stage, and CT scan sufficient? Abiraterone has a benefit in very high risk localized prostate cancer (median PSA 35 ng/mL), as well as benefit in low and high volume mHSPC. Radiotherapy to the primary has benefit in high risk localized prostate cancer, as well as benefit in low volume and potentially high volume mHSPC. Dr. Spratt also notes that experts cannot agree on what a bone scan shows, with an inter-reader agreement for bone scan being moderate (Fleiss k 0.51). Based on work from Australia, early adoption of PSMA PET/CT suggests that bone scan is already dead:
Moreover, even among late adopters to PSMA PET/CT, work from New York suggests that bone scan is also already dead, with utilization dropping from 100% to 25% in 2.5 years:
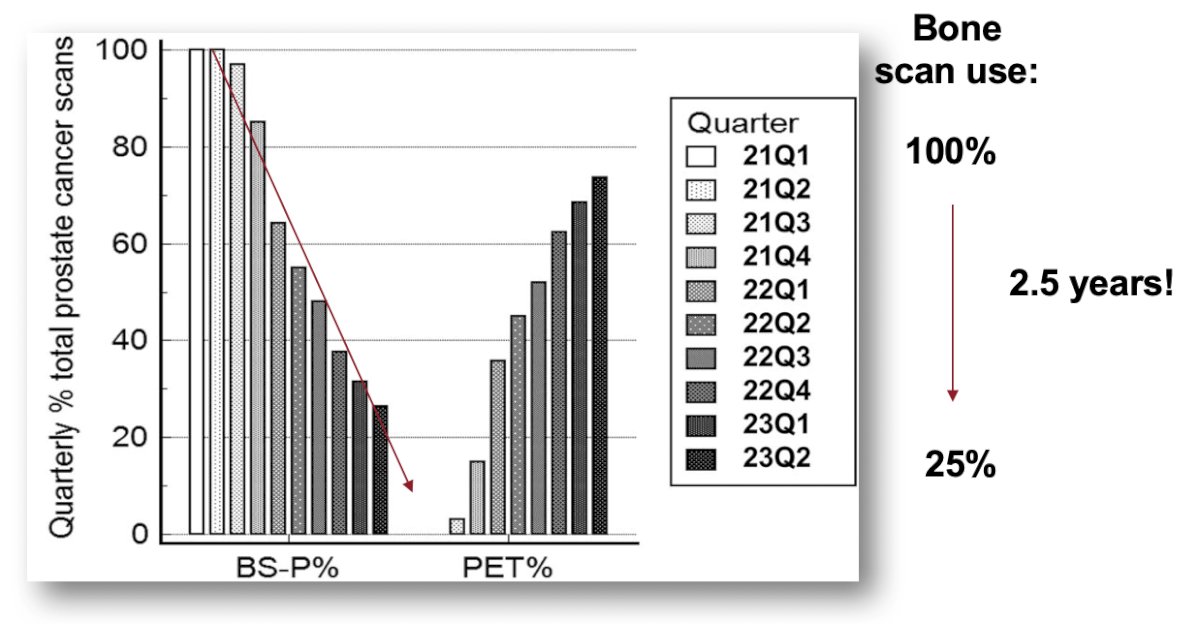
Dr. Spratt concluded his presentation discussing whether we can kill the bone scan by emphasizing that it is already dead. Hence, why we are not at the 2025 Bone Scan conference.
Presented by: Daniel Spratt, MD, University Hospitals, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:- Singh KB, London KI, Wong VCK, et al. Diagnostic accuracy of bone scan at different PSA levels in biochemical recurrence of prostate cancer. J Med Imag Rad Sci. 2024;55(1):91.96.
- Hofman MS, Lawrentschuk N, Francis, RJ, et al. Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): A prospective, randomized, multicentre study. Lancet 2020 Apr 11;395(10231):1208-1216.
- Cher MI, Bianco Jr FJ, Lam JS, et al. Limited role of radionuclinde bone scintigraphy in patients with prostate specific antigen elevations after radical prostatectomy. J Urol. 1998 Oct;160(4):1387-1391.
- Gomez P, Manoharan M, Kim SS, et al. Radionuclide bone scintigraphy in patients with biochemical recurrence after radical prostatectomy: when is it indicated? BJU Int. 2004 Aug;94(3):299-302.
- Holzgreve A, Armstrong WR, Clark KJ, et al. PSMA-PET/CT findings in patients with high-risk biochemically recurrent prostate cancer with no metastatic disease by conventional imaging. JAMA Netw Open. 2025 Jan 2;8(1):e2452971.