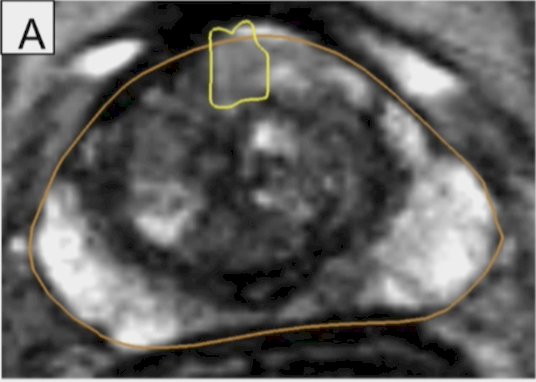
(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a PSMA session and a presentation by Dr. Wayne Brisbane discussing whether PSMA-targeted prostate biopsy can detect cancer when MRI-guided biopsy is negative. To date, MRI guided biopsy is the standard of care, however, MRI misses prostate cancer in 7-12% of cases, in addition to targeted biopsies potentially missing tumor targets. Dr. Brisbane started with a case discussion of a 71 year old male on active surveillance who in 2009 had a negative prostate biopsy at a PSA of 2.6 ng/mL. In 2012, he underwent another biopsy, which was benign, and in 2012 he also underwent a TURP (benign pathology). In 2013, he had a third prostate biopsy, which showed Gleason 3+3 prostate cancer (0.5 mm) at a PSA of 8.5: His MRI showed a PIRADS 2 lesion as follows:
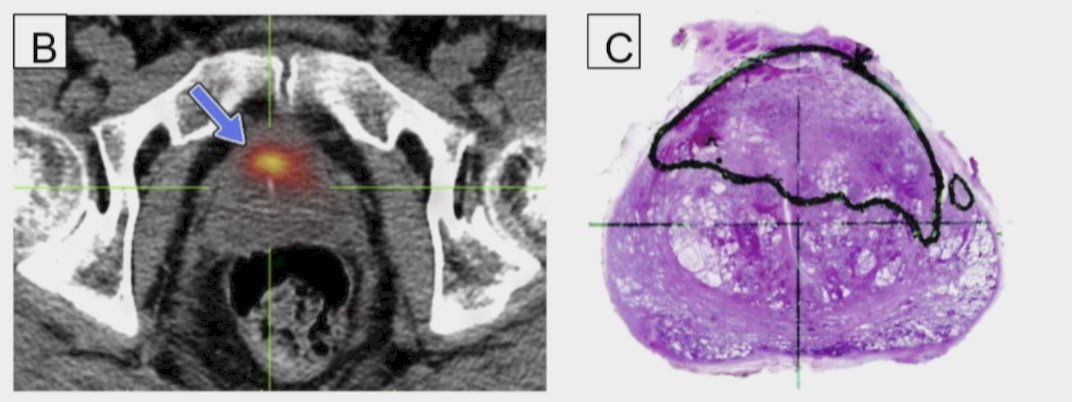
Notably, a subsequent PSMA PET showed a specific lesion in the prostate, which was found to be Gleason 3+4 (40%), with mucinous features:
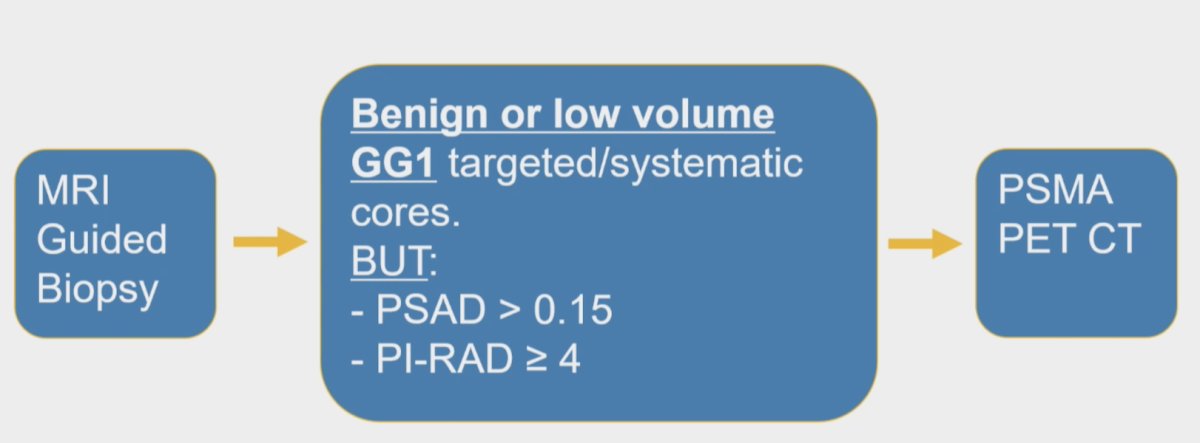
The objective of their study at UCLA was to undertake a phase 1 trial to assess the detection rate of Grade Group 2+ prostate cancer in patients with 68Ga-PSMA-11 uptake in the prostate following benign or low volume Gleason Group 1 MRI guided biopsy. The trial design is as follows:
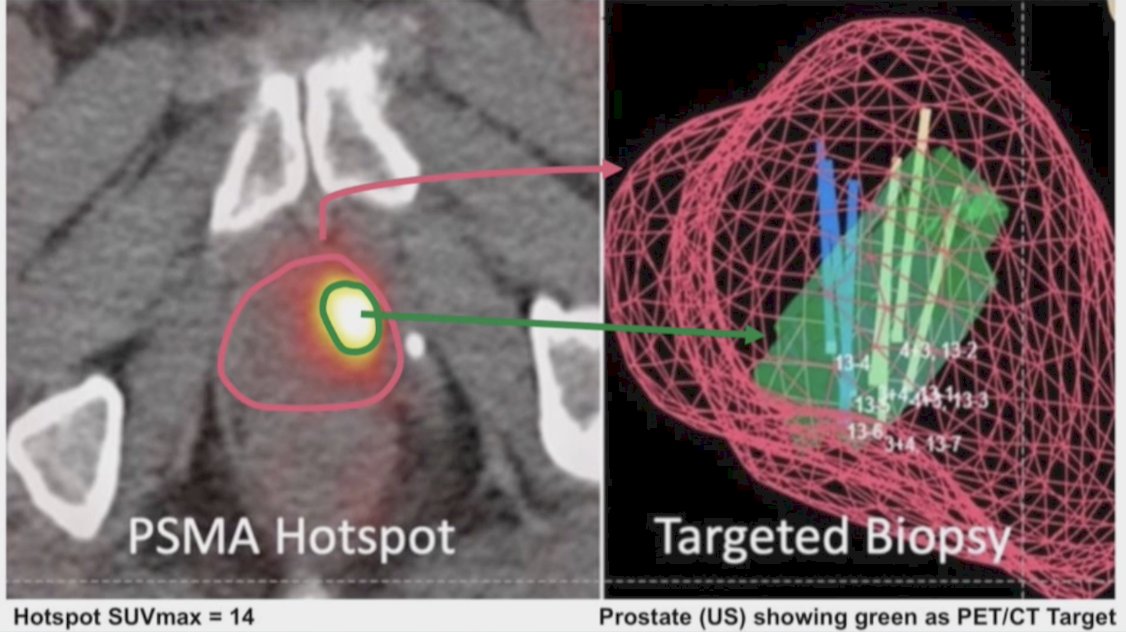
Overall, 70 patients underwent a PSMA PET/CT, with 31 patients undergoing observation for a PSMA lesion SUVmax < 3, and 39 patients undergoing PSMA guided fusion biopsy for a PSMA lesion SUVmax 3+:
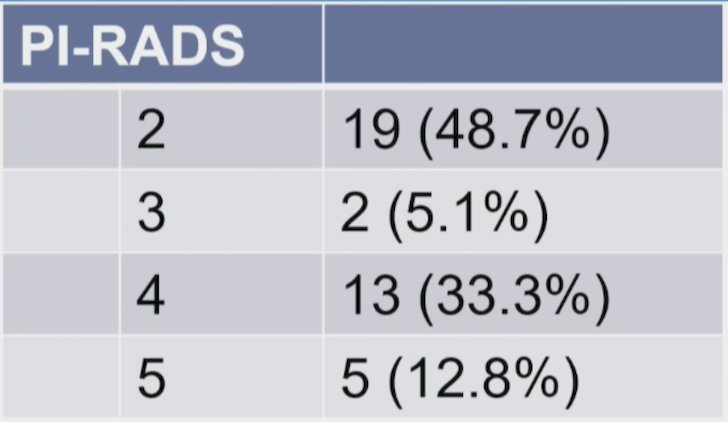
Among these 39 patients, the median age was 64 years, 87% had initial no prostate cancer, with the following PIRADS delineation:
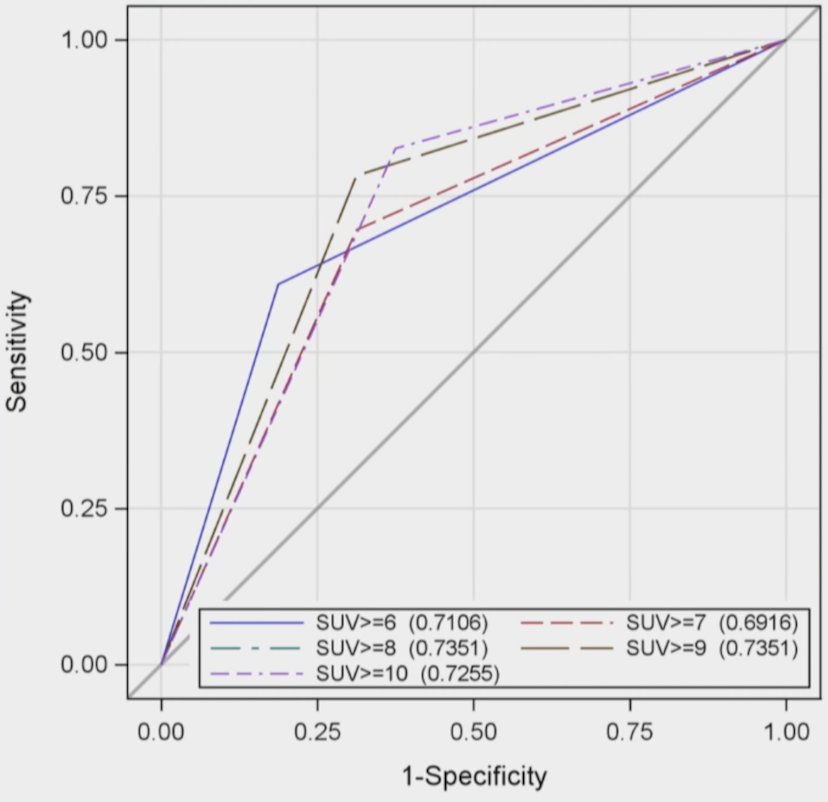
Among the 16 patients (41%; 16/39) biopsied with Gleason Group 2+ prostate cancer, 6 were Gleason Group 2, 5 were Gleason Group 3, 3 were Gleason Group 4, and 2 were Gleason Group 2. There were 5/16 patients with prior MRI lesions and 11/16 with no de novo MRI lesions. Among the 5 patients with MRI concordant PSMA lesions, there was a similar distribution between MRI and PSMA cancer-containing regions of interest. For MRI discordant or de novo PSMA regions of interest, the results based on SUVmax and Gleason Grade are as follows:

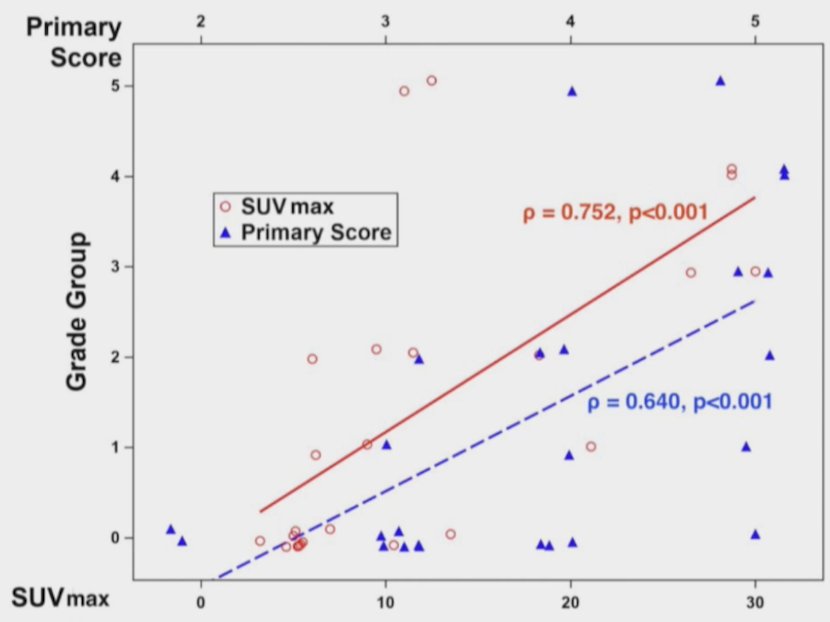
The correlation between SUVmax and PRIMARY score was 0.75 (p < 0.001) for SUVmax and 0.64 (p < 0.001) for the PRIMARY score:
PIRADS and PSA density did not significantly influence biopsy results (p > 0.05).
Dr. Brisbane concluded his presentation by discussing whether PSMA-targeted prostate biopsy can detect cancer when MRI-guided biopsy is negative with the following take home points:
- Following a negative MRI guided biopsy, PSMA provides a ‘second look’, providing:
- Risk stratification: SUV <= 7 excludes most significant cancers
- Anatomic information: 28% are de novo Gleason Group 2+ lesions, and 12.8% missed MRI positive lesions
- Future work should validate and expand this application for PSMA PET
Presented by: Wayne Brisbane, MD, University of California, Los Angeles, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.