(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a PSMA session and a presentation by Dr. Irene Buvat discussing whole body PSMA quantitative parameters and why we are not using them in the real world. Dr. Buvat notes that there are several clinically valuable whole body quantitative features in PSMA PET, which include:
- The number of tumor sites
- SUVmean calculated over all whole body tumors
- Total tumor volume
- Organ-specific tumor volume
Of note, all of these features require whole body tumor segmentation. However, currently, one push button whole body tumor segmentation is not widely available. Dr. Buvat notes that one surrogate for whole body features is visual scores. Gafita et al.1 previously assessed the agreement of RECIP determined using tumor segmentation software (quantitative RECIP) with RECIP determined by qualitative reads by nuclear medicine physicians (visual RECIP) for response evaluation in metastatic castration-resistant prostate cancer. Among 124 men included in this study, agreement between visual versus quantitative RECIP was excellent (κ = 0.89; 118 of 124 men [95%]). Agreement among readers in classifying visual RECIP progressive disease versus non-progressive disease was also excellent (κ = 0.81; 103 of 124 men [83%]).
In 2025, Dr. Buvat states that the time has come for automated segmentation and that it will be a game changer:
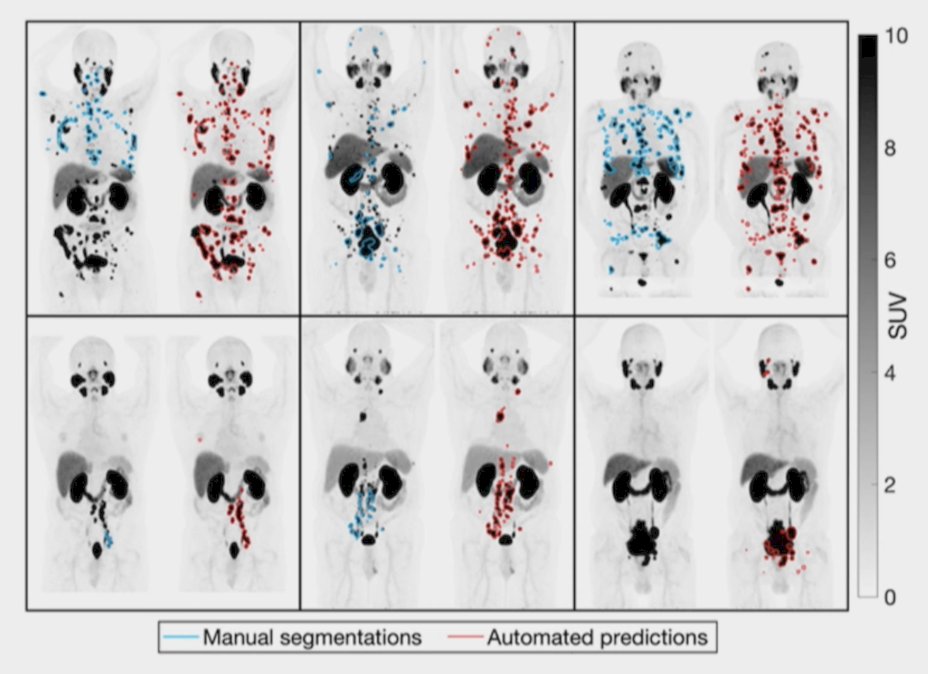
She does caution, however, that not all artificial intelligence solutions yield the same segmentation results, given that different segmentation methods (artificial intelligence based or not) often yield different contours:
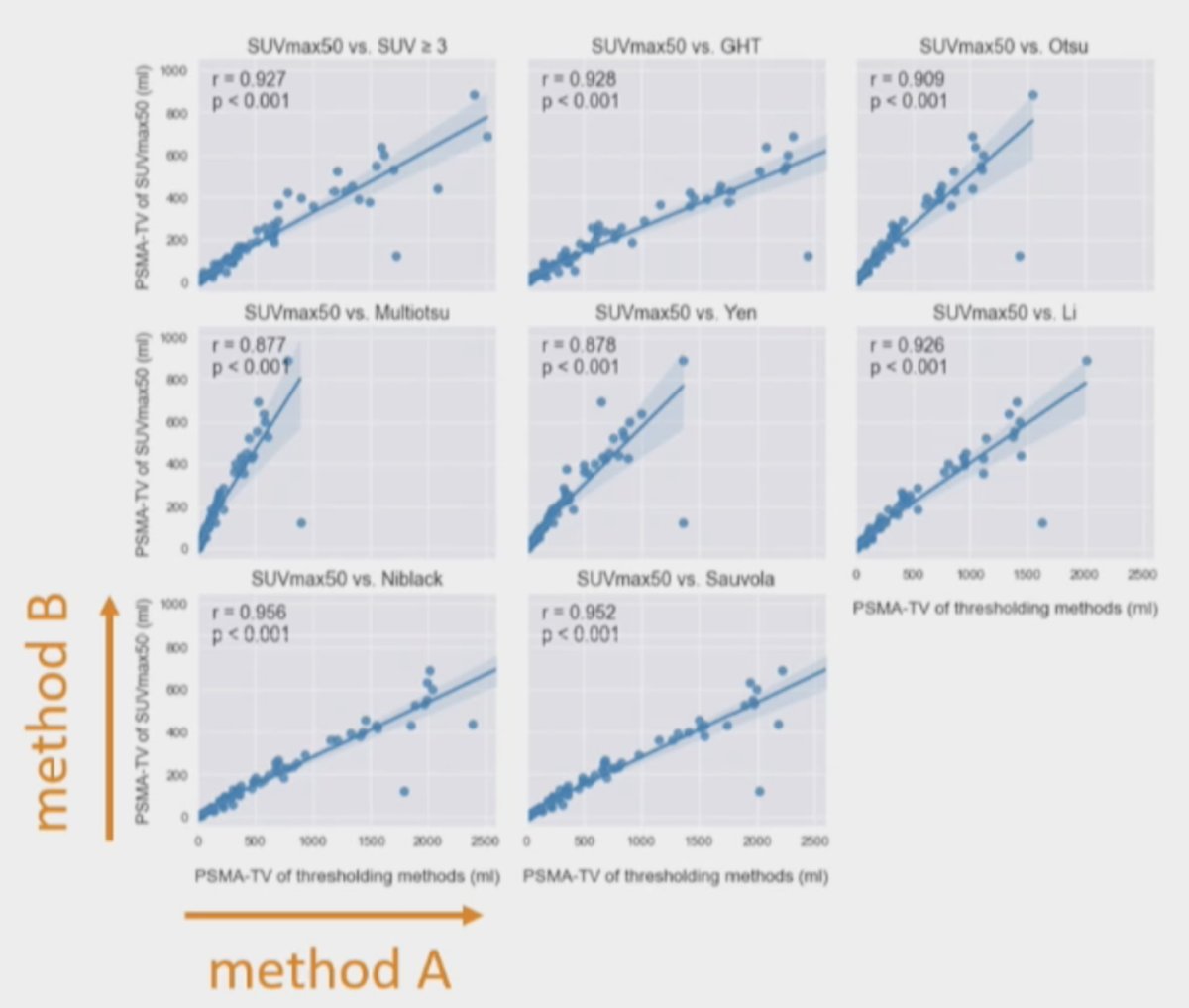
The artificial intelligence based segmentation method does matter, given that different artificial intelligence solutions produce different results (total tumor volume, SUVmean, etc). It is difficult to agree on consensus cutoff values for decision making, for example, a SUVmean > 10. A benchmark needs to be created, a standard against which something is compared. One way is for publically shared PSMA PET/CT scans, with a broad variety of uptake patterns, taken together with consensus segmentation and total tumor volume for each. This way anyone can check that his/her artificial intelligence tool yields the correct values.
Discussing work from her own group, they recently developed an international benchmark for total metabolic tumor volume measurement in baseline 18F-FDG PET/CT of lymphoma patients.3 Total metabolic tumor volume was measured by 12 nuclear medicine experts, each analyzing 20 cases split across subtypes, with each case processed by 3-4 readers. They found that the final total metabolic tumor volume ranged from 8 to 2,288 cm3, showing excellent agreement among all readers in 87% of cases with a difference of less than 10% or less than 10 cm3 in 70% of the cases.
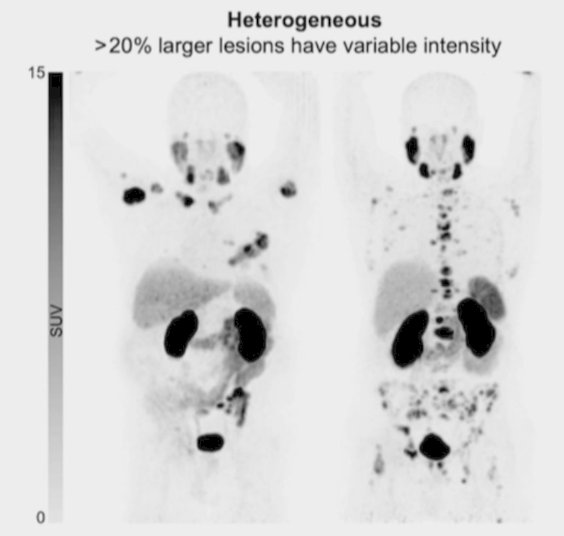
An additional benefit of automated segmentation is that plenty of candidate prognostic/predictive biomarkers can be systematically explore. For example, heterogeneity of tumor uptake, and percent volume showing response:
Furthermore, automated segmentation also becomes available for FDG PET, whereby a fraction of total tumor volume (by FDG PET) is PSMA positive. Also, PET segmentation + CT whole body segmentation (ie. using TotalSegmentator) more automatically calculates candidate biomarkers (ie. tissue-specific tumor volume).
Dr. Buvat concluded her presentation by discussing whole body PSMA quantitative parameters and why we are not using them in the real world with the following take home points:
- The time has come to shift to artificial intelligence driven tumor segmentation (even if it is not yet perfect) to leverage quantitative whole body PSMA imaging
- We need to create and agree on a benchmark
- We should assess “one push button” artificial intelligence tools
- We need to systematically generate whole body biomarkers (ie. total tumor volume)
- The most clinically useful whole body biomarkers will naturally emerge
Presented by: Irene Buvat, PhD, Institut Curie, Orsay, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Gafita A, Djaileb L, Rauscher I, et al. Response evaluation criteria in PSMA PET/CT (RECIP 1.0) in metastatic castration-resistant prostate cancer. Radiology. 2023 Jul;308(1):e222148.
- Leung KH, Rowe SP, Sadaghiani MS, Leal JP, Mena E, Choyke PL, Du Y, Pomper MG. Deep Semisupervised Transfer Learning for Fully Automated Whole-Body Tumor Quantification and Prognosis of Cancer on PET/CT. J Nucl Med. 2024;65(4):643–50.
- Boellaard R, Buvat I, Nioche C, et al. International benchmark for total metabolic tumor volume measurement in baseline 18F-FDG PET/CT of lymphoma patients: A milestone toward clinical implementation. J Nucl Med. 2024 Sep 3;65(9):1343-1348.