(UroToday.com) The 2025 PSMA and Beyond annual meeting featured a LuPSMA therapy session and a presentation by Dr. Tanya Dorff discussing treatment sequencing with radioligand therapy in mCRPC. According to the NCCN guidelines, there is no single path for treatment mCRPC:

There are several important considerations for sequencing treatment for patients:
- What will be the most effective treatment?
- Is there a biomarker to help with selecting treatment?
- What are the side effects of treatment?
- Is there concern for cross resistance?
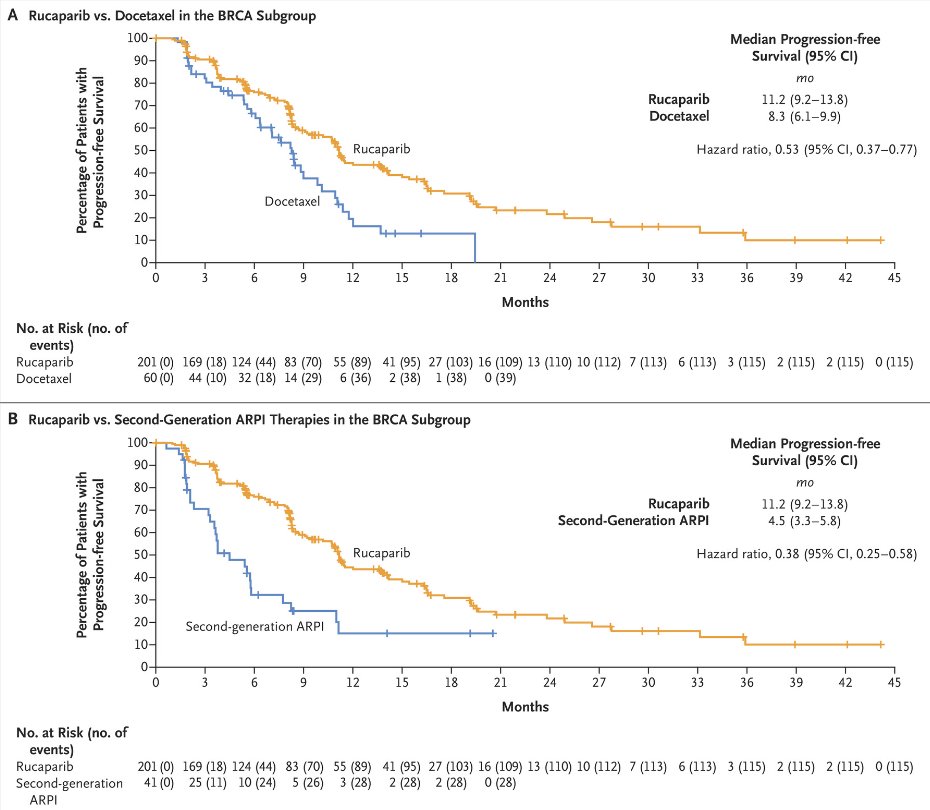
TRITON-3 [1] previously assessed PARP inhibitors versus chemotherapy for HRR alterations, but what about radioligand therapy? Among patients with BRCA alterations, TRITON-3 showed that these patients do better with rucaparib than docetaxel, but the docetaxel radiographic progression free survival was shorter than in unselected populations (ie. 12 months in FIRSTANA [2]):
In a recent study from Wenzel et al. [3], they assessed progression-free survival and overall survival rates of patients with mCRPC with BRCA or tumor suppressor gene mutations (TP53, PTEN, RB1). Among 194 mCRPC patients, 22% had BRCA1/2 alterations versus 14% with PTEN/TP53/RB1 versus 63% without one of these mutations. Of 87 patients with 177Lu-PSMA-617 treated mCRPC, there were significant differences in progression free survival and overall survival observed (both p ≤ 0.02). The following shows the Kaplan Meier curve for progression free survival:

Based on the PSMAfore trial [4], perhaps 177Lu-PSMA-617 should be considered before docetaxel chemotherapy. The trial design for PSMAfore is noted below:

Dr. Dorff emphasized the median radiographic progression free survival was 12.02 months in the 177Lu-PSMA-617 arm versus 5.59 months in the androgen receptor pathway inhibitor change arm (HR 0.43, 95% CI 0.33-0.54).
What about 177Lu-PSMA-617 versus radium-223? The RaLu [5] study reported that 177Lu-PSMA-617 can be safely administered after radium-223, however similar data is not yet available for radium-223 after 177Lu-PSMA-617. Thus, Dr. Dorff notes that perhaps we should use radium with bone only disease, prior to visceral involvement. Or should we use radium-223 after visceral metastases are all treated with PSMA radioligand therapy?
For considering 177Lu-PSMA-617 versus cabazitaxel, Dr. Dorff discussed the TheraP trial [6], which showed a greater PSA response with radioligand therapy and a greater pain response (60% versus 43%):

There were fewer grade 3+ treatment emergent adverse events (33% versus 53%) with radioligand therapy. Specific grade 3+ adverse events included thrombocytopenia 11% with radioligand therapy versus 0% with cabazitaxel,and febrile neutropenia 0% with radioligand therapy versus 8% with cabazitaxel. The median radiographic progression was 5.1 months versus 5.1 months (HR favoring 177Lu-PSMA-617 0.64, 95% CI 0.46-0.88):

The following table highlights the differences between the TheraP and VISION [7] trials:

Dr. Dorff concluded her presentation by discussing treatment sequencing with radioligand therapy in mCRPC by highlighting what the optimal sequence may look like:
- Biopsy progression when possible (especially visceral metastases)
- Repeat next generation sequencing (ie. with ctDNA) for new actionable mutations at least once
- If there is an HRR alteration, we should use PARP inhibitors earlier
- If there is an MSI high mutation or high tumor mutational burden we should consider pembrolizumab first
- If there is symptomatic, rapid progression we should be considering chemotherapy or radioligand therapy:
- Is PSMA PET the deciding factor?
- Heterogeneity upon CRPC progression may favor earlier use of radioligand therapy
- For low volume, asymptomatic patients, immunotherapy, BAT, and/or clinical trials with androgen receptor pathway inhibitor switch may be ideal
Presented by: Tanya Dorff, MD, City of Hope, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 PSMA and Beyond Annual Meeting, Los Angeles, CA, Fri, Mar 28 – Sat, Mar 29, 2025.
References:
- Fizazi K, Piulats JM, Reaume MN, et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N Engl J Med. 2023 Feb 23;388(8):719-732.
- Oudard S, Fizazi K, Sengelov L, et al. Cabizitaxel versus Docetaxel as first-line therapy for patients with metastatic castration-resistant prostate cancer: A randomized phase III Trial-FIRSTANA. J Clin Oncol 2017;35(28):3189-3197.
- Wenzel M, Koll F, Hoeh B, et al. Cancer-control outcomes of patients with metastatic castration-resistant prostate cancer with BRCA gene or tumor suppressor mutations undergoing 177-Lutetium Prostate-Specific Membrane Antigen Radioligand Therapy. JCO Precis Oncol. 2024 Dec 6 [Epub ahead of print].
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Rahbar K, Essler M, Pabst KM, et al. Safety and Survival Outcomes of 177Lu-Prostate-Specific Membrane Antigen Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer with Prior 223Ra Treatment: The RALU Study. J Nucl Med. 2023 Apr;64(4):574-578.
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.