(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer late-breaking abstract (LBA) session. Dr. Siamak Daneshmand presented the 1-year disease-free survival (DFS) results from SunRISe-1 evaluating the gemcitabine intravesical system (Gem-iDRS), INLEXZO™ (gemcitabine intravesical system; formerly TAR-200), as monotherapy in patients with BCG-unresponsive, papillary-only, high-risk, non-muscle invasive bladder cancer (NMIBC).
There is a substantial unmet need in this population, with Dr. Daneshmand noting that approximately 75% of bladder cancers are NMIBC, and nearly half meet criteria for high-risk disease.1 Recurrence or progression despite BCG occurs in ~50% of HR NMIBC cases,3-5 yet papillary-only BCG-unresponsive disease has no FDA-approved bladder-sparing therapies. Treatment options are limited, and radical cystectomy—while guideline-supported—carries significant morbidity, quality-of-life impact, and mortality rates ranging from 3% to 8%.2,6-8 Investigational therapies are being explored, but recent 12-month disease-free (DFS) and recurrence-free survival (RFS) rates range between 44% and 55% only.9–11

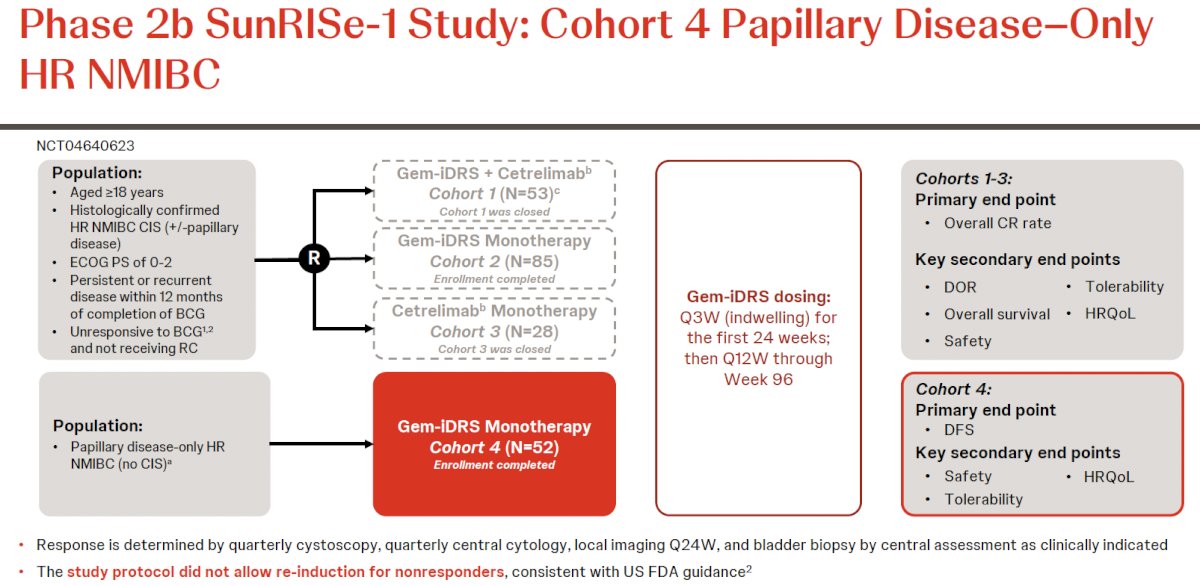
Gem-iDRS (INLEXZO) provides sustained gemcitabine delivery throughout all layers of the bladder wall and was recently approved for BCG-unresponsive CIS with or without papillary disease.12–14 Cohort 4 of SunRISe-1 specifically enrolled patients with high-grade Ta or T1 papillary-only disease, excluding CIS, with BCG-unresponsive status confirmed per FDA guidance. The primary endpoint was 12-month DFS, defined by centrally adjudicated recurrence, progression, or death. The protocol did not allow re-induction for non-responders.
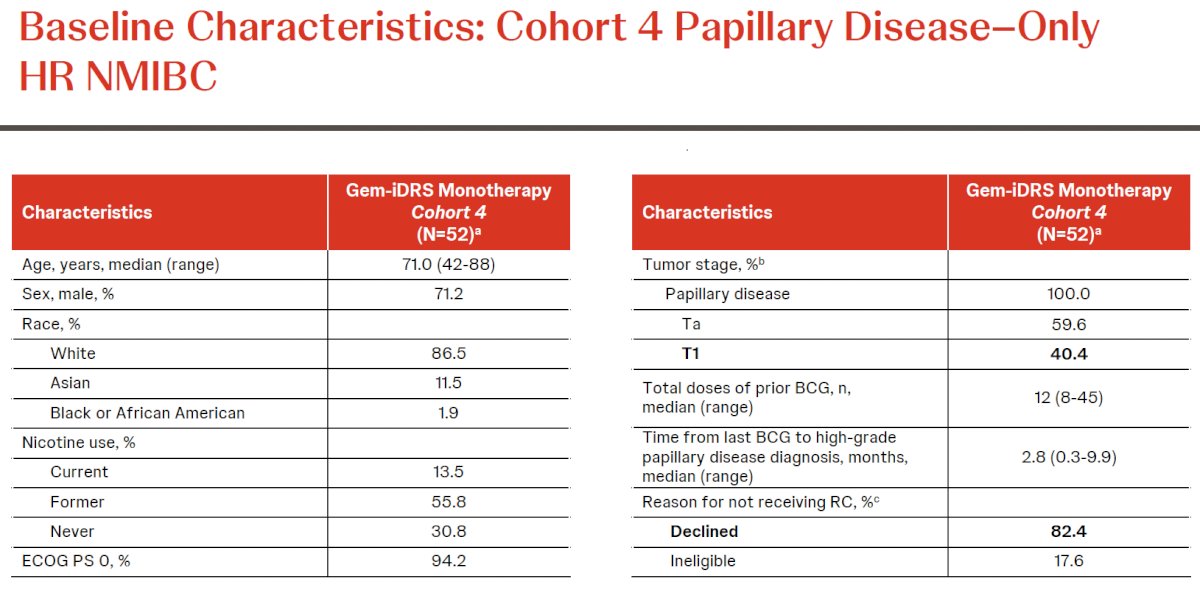
A total of 52 patients received at least one dose of Gem-iDRS. The median age was 71 years (range 42–88), and 71.2% were male. Most had prior BCG exposure with a median of 12 instillations (range 8–45). Tumor staging included 59.6% with HG Ta and 40.4% with T1 disease. The median time from last BCG to papillary recurrence was 2.8 months. Declining cystectomy was the most common reason for surgical ineligibility (82.4%).
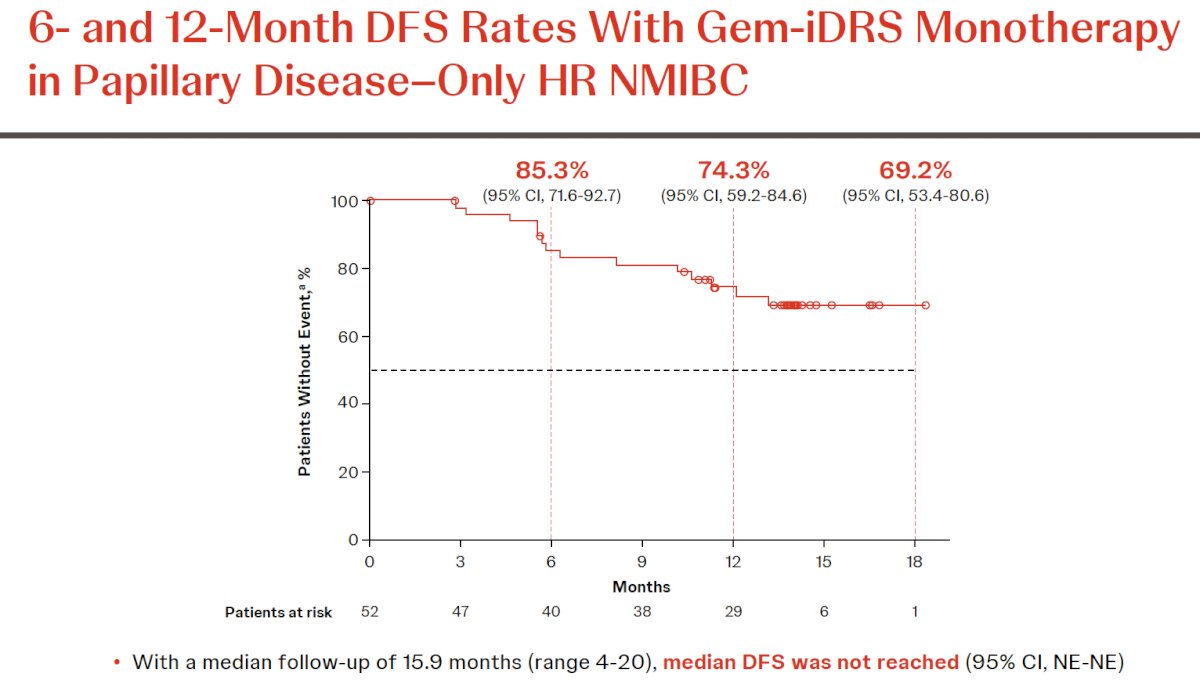
With a median follow-up of 15.9 months, median DFS was not reached. The 6- and 12-month DFS rates were 85.3% and 74.3%, respectively.
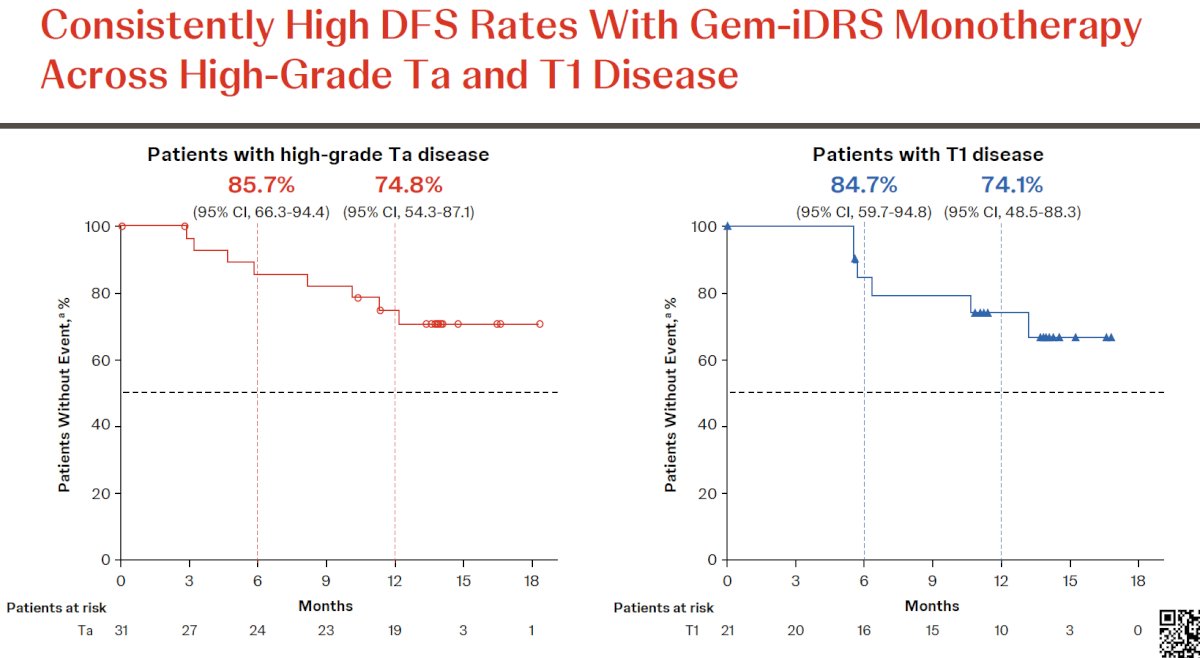
DFS rates were consistent across stage subsets. In patients with HG Ta disease, 6- and 12-month DFS rates were 85.7% and 74.8%. In T1 patients, the corresponding DFS rates were 84.7% and 74.1%.
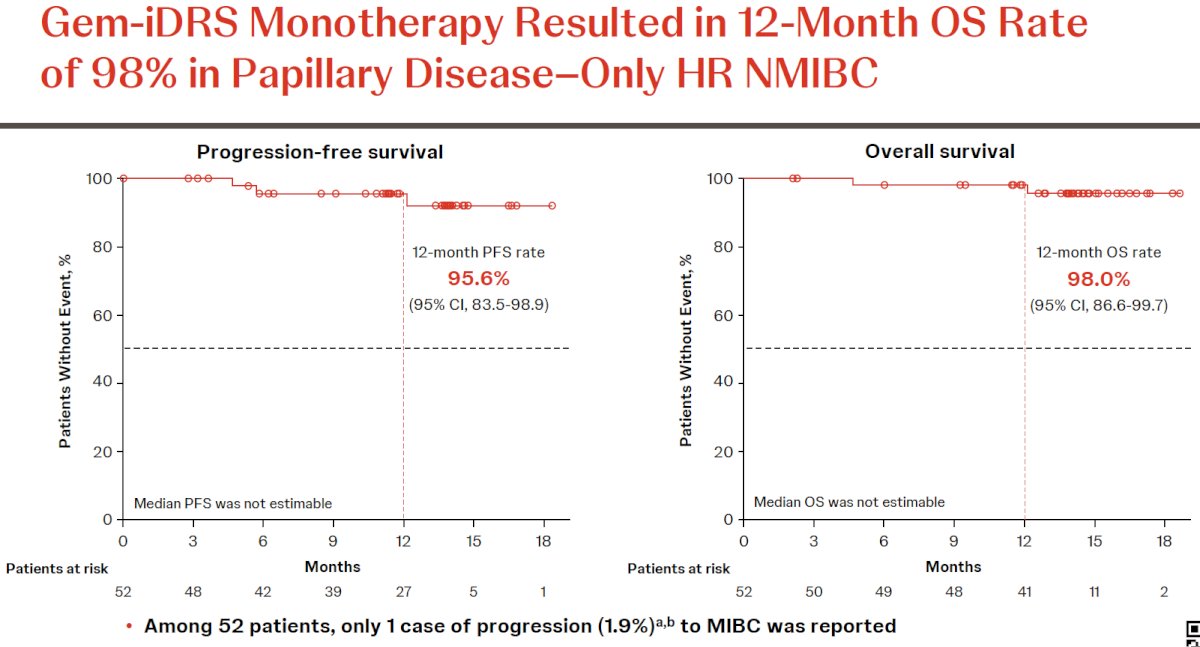
Progression events were rare. Only one patient (1.9%) progressed to MIBC. Twelve-month PFS was 95.6%. Overall survival at 12 months was 98%.
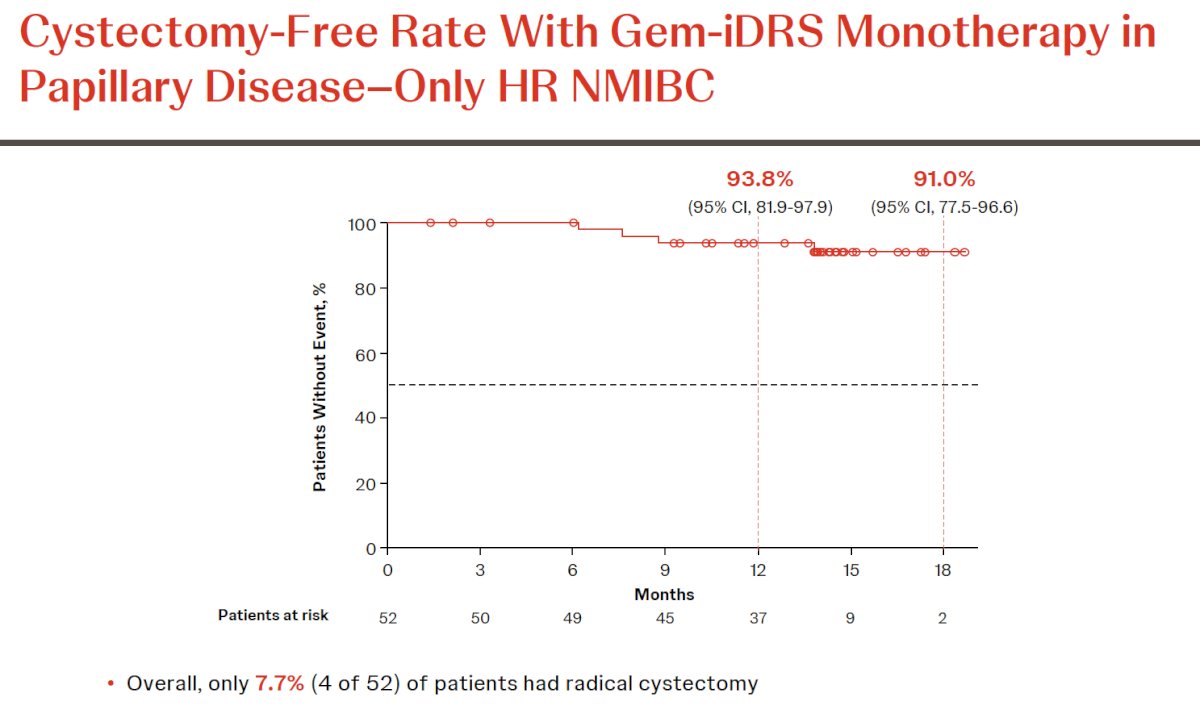
Radical cystectomy was performed in only 4 of 52 patients (7.7%). Cystectomy-free survival at 12 months was 91%.
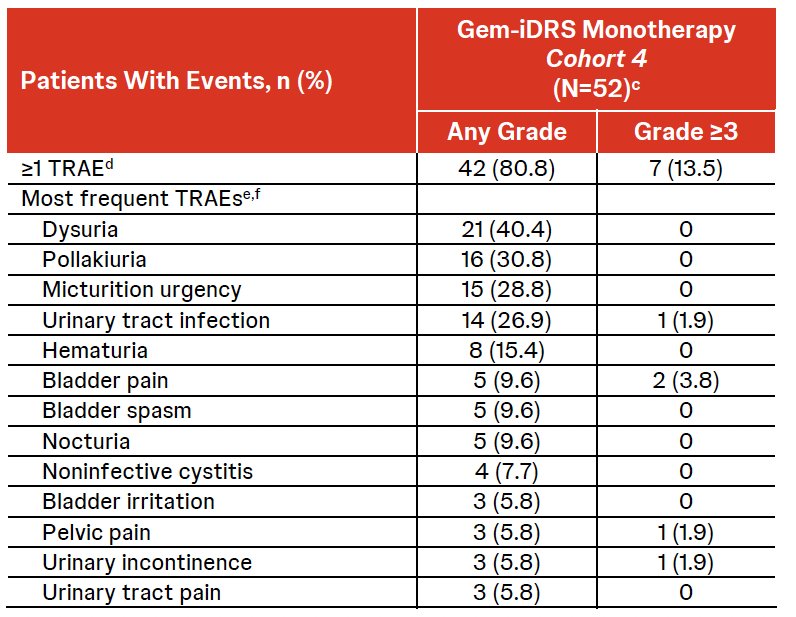
Gem-iDRS was well tolerated. Among 52 treated patients, 80.8% experienced at least one treatment-related adverse event (TRAE), nearly all Grade 1–2. Grade ≥3 TRAEs occurred in 13.5%. The most frequent TRAEs included dysuria (40.4%), pollakiuria (30.8%), micturition urgency (28.8%), urinary tract infection (26.9%), hematuria (15.4%), and bladder pain (9.6%). Serious TRAEs occurred in three patients (5.8%). Four patients (7.7%) discontinued due to TRAEs. Importantly, no treatment-related deaths occurred, and insertion success was 99.8% (419/420). The median AE resolution time was 3.3 weeks.
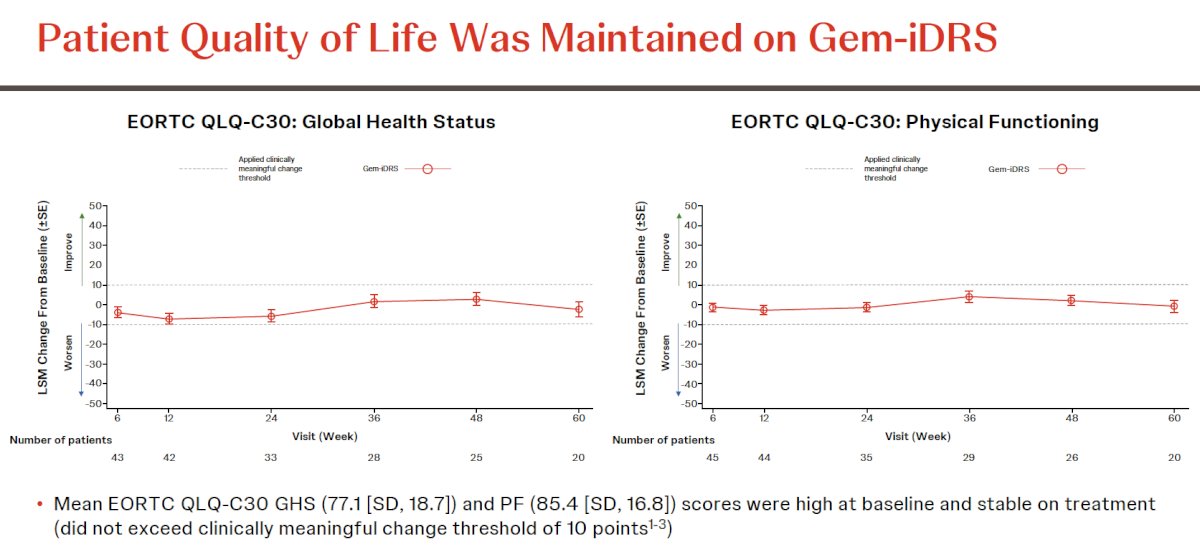
Quality-of-life outcomes were preserved. Mean EORTC QLQ-C30 global health status (77.1, SD 18.7) and physical functioning (85.4, SD 16.8) scores were high at baseline and remained stable throughout treatment without exceeding the 10-point threshold for clinically meaningful deterioration.1–3
Dr. Daneshmand concluded as follows:
- Gem-iDRS (TAR) monotherapy demonstrated a high 12-month disease-free survival rate in BCG-unresponsive papillary disease–only HR NMIBC
- 12-month DFS rate was 74.3%
- DFS rates were consistently high across both high-grade Ta and T1 disease
- At 12 months, nearly all patients were alive (OS rate: 98%) and did not have progression (PFS rate: 95.6%)
- Only 4 of 52 patients (7.7%) underwent subsequent radical cystectomy
- Gem-iDRS was well tolerated, with low rates of serious TRAEs and discontinuations due to TRAEs
- Overall health status and high physical functioning were maintained while on Gem-iDRS treatment
- The phase 3 randomized SunRISe-5 study (NCT06211764) of Gem-iDRS versus intravesical chemotherapy is investigating Gem-iDRS as a potential bladder-sparing therapy in BCG-unresponsive/-experienced papillary-only HR NMIBC
Presented by: Siamak Daneshmand, MD, Professor of Urology, Department of Urology, University of Southern California, Los Angeles, CA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
References:
- Sylvester RJ, van der Meijden APM, Lamm DL, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables. Eur Urol. 2006;49:466–475.
- Cumberbatch MGK, Foerster B, Catto JWF, et al. Epidemiology of bladder cancer: Diagnosis, staging, and survival. Eur Urol. 2018;74(6):784–795.
- Kamat AM, Li R, O’Donnell MA, et al. Predicting response to intravesical BCG therapy using clinical and tumor characteristics in high-risk non–muscle invasive bladder cancer. J Clin Oncol. 2016;34(16):1935–1944.
- Lenis AT, Lec PM, Chamie K, Mshs MD. Bladder cancer: a contemporary update on epidemiology, molecular characterization, and therapy. Nat Rev Urol. 2020;17:251–264.
- Brausi M, Oddens J, Sylvester R, et al. Side effects and treatment withdrawal in intravesical BCG therapy for NMIBC: Results from the EORTC Genito-Urinary Group. Eur Urol. 2014;65(1):69–76.
- Cambier S, Sylvester RJ, Collette L, et al. EORTC nomograms and risk groups for predicting recurrence and progression in non–muscle invasive bladder cancer. Eur Urol. 2016;69(1):60–69.
- Martínez-Pineiro L, Portillo JA, Fernández JM, et al. Maintenance BCG therapy in high-risk NMIBC: outcome and adverse events. J Urol. 2015;193:14–19.
- Holzbeierlein JM, Cookson MS, Weiner AB, et al. National impact of the BCG shortage on NMIBC treatment patterns and outcomes. J Urol. 2024;10.1097/JU.0000000000003846.
- Maibom SL, Møller H, Vedsted P, et al. Early complications, readmissions, and mortality after radical cystectomy: A population-based study. BMJ Open. 2021;11(4):e043266.
- Clements M, Foster C, Witherspoon L, et al. Patient-reported outcomes and quality of life following radical cystectomy: A contemporary evaluation. Eur Urol. 2021;81(3):294-304.
- Steinberg RL, Thomas LJ, Nepple KG, et al. Sequential intravesical gemcitabine and docetaxel for BCG-unresponsive NMIBC: Real-world multi-institutional outcomes. J Urol. 2020;203(5):902–909.
- Daneshmand S, Kamat AM, O’Donnell MA, et al. TAR-200 intravesical gemcitabine device in BCG-unresponsive NMIBC: Clinical and biological insights from the SunRISe program. J Clin Oncol. 2025;JCO2501651.
- Shore ND, Cookson MS, Amling CL, et al. Novel intravesical therapies for NMIBC: Current evidence and future directions. Urol Oncol. 2023;41(2):73–84.
- Tyagi P, Li J, Lim J, et al. Pharmacokinetics and tissue penetration of sustained-release gemcitabine delivery systems in the bladder. Clin Cancer Res. 2022;28:1123–1131.