(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer poster session. Dr. Girish Kulkarni presented an ad hoc analysis of the phase 2b SunRISe-1 Trial evaluating baseline urinary tumor DNA (utDNA), minimal residual disease (MRD), and genomic disease burden in relation to clinical response to INLEXZO™ (gemcitabine intravesical system; formerly TAR-200).
For patients with high-risk, non-muscle invasive bladder cancer (HR NMIBC), intravesical therapy with bacillus Calmette-Guérin (BCG) is the standard-of-care treatment.1 However, one third of patients become unresponsive to BCG, with >50% experiencing recurrence and progression during long-term follow-up.2,3 Gemcitabine intravesical system (gem iDRS; INLEXZO™) is an intravesical drug-releasing system designed to provide sustained local delivery of gemcitabine in the bladder.
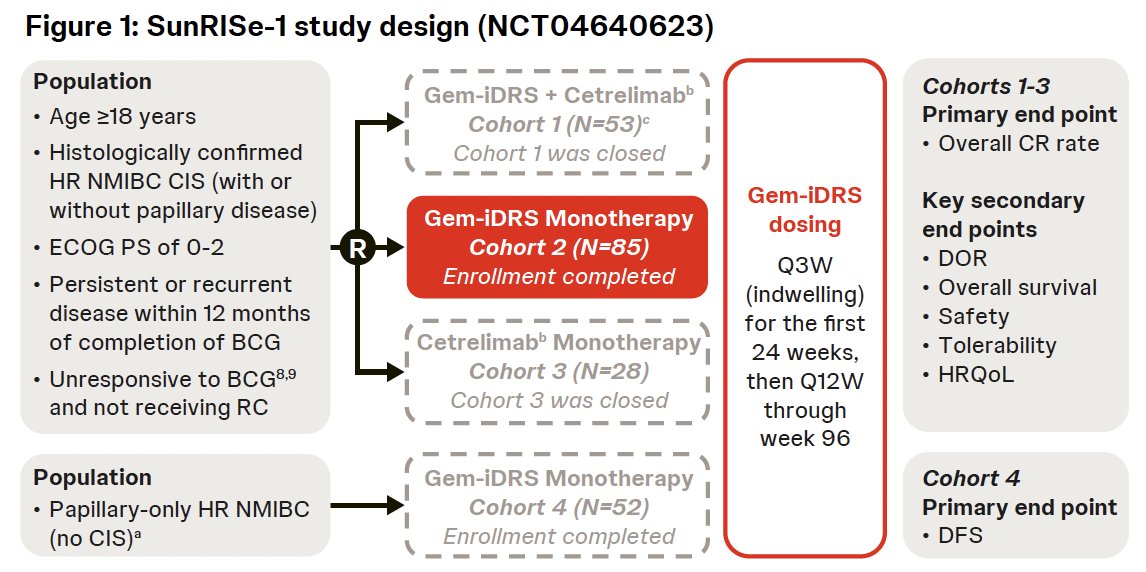
Cohort 2 of the ongoing phase 2b SunRISe-1 study is assessing the efficacy and safety of gem-iDRS monotherapy in patients with BCG-unresponsive HR NMIBC with carcinoma in situ (CIS) ± papillary disease. The primary analysis of SunRISe-1 Cohort 2 demonstrated a clinically significant efficacy and a positive benefit-risk profile for gem iDRS monotherapy.4 utDNA status detects MRD with high sensitivity in patients with BCG‑unresponsive NMIBC.5,6 The study objective was to assess the baseline utDNA status and its association with response to gem-iDRS monotherapy in patients with BCG-unresponsive HR NMIBC with CIS ± papillary disease.
Urine-based Genomic Profiling
Urinary MRD analysis was conducted for the gem-iDRS monotherapy cohort. Pretreatment residual urine cytology pellets were tested using UroAMP assay (Convergent Genomics, South San Francisco, CA)7. utDNA MRD status was classified using a locked logistic regression model with mutation profiles as input features. The genomic disease burden (GDB) was defined as the percentile rank of the sum of variant allele frequency of all somatic mutations in a sample among the empirical distributions of NMIBC utDNA samples. Genomic data from baseline urine samples were available from 41 of 85 patients in Cohort 2.
Overview of Patients Included in utDNA Analysis
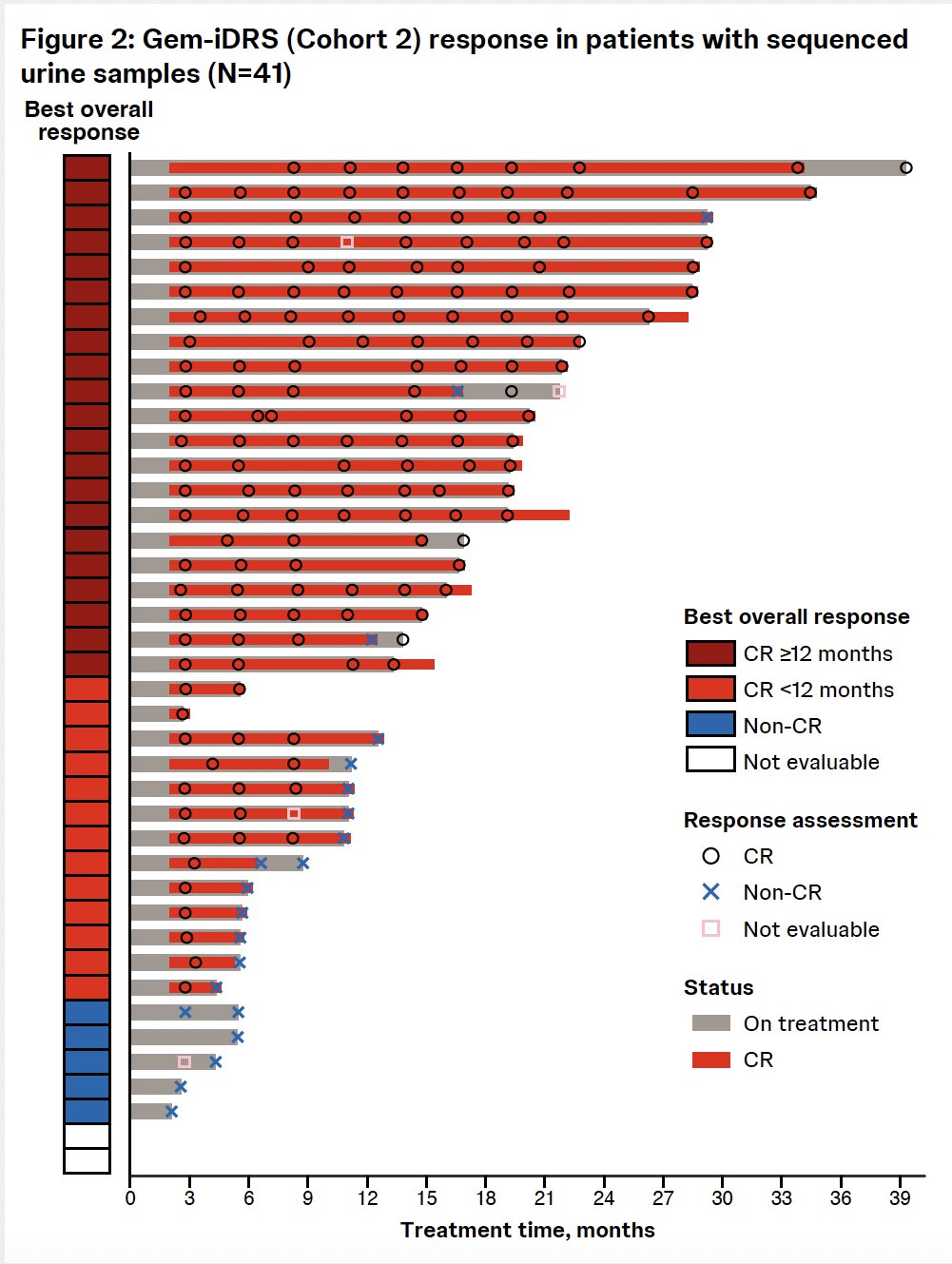
This analysis included 41 patients treated with gem-iDRS monotherapy in SunRISe-1 Cohort 2 who had available utDNA MRD results. Notably, 34 of 41 patients (83%) achieved a CR at any time. Of the 34 responders, 21 had CR ≥12 months.
At baseline, 23/41 (56%) patients were utDNA MRD positive (+) and 18/41 (44%) were MRD negative (-). Of both MRD+ and MRD- patients, the majority were male and had CIS only (no papillary disease). The baseline utDNA MRD status was independent of patient demographics and disease characteristics.
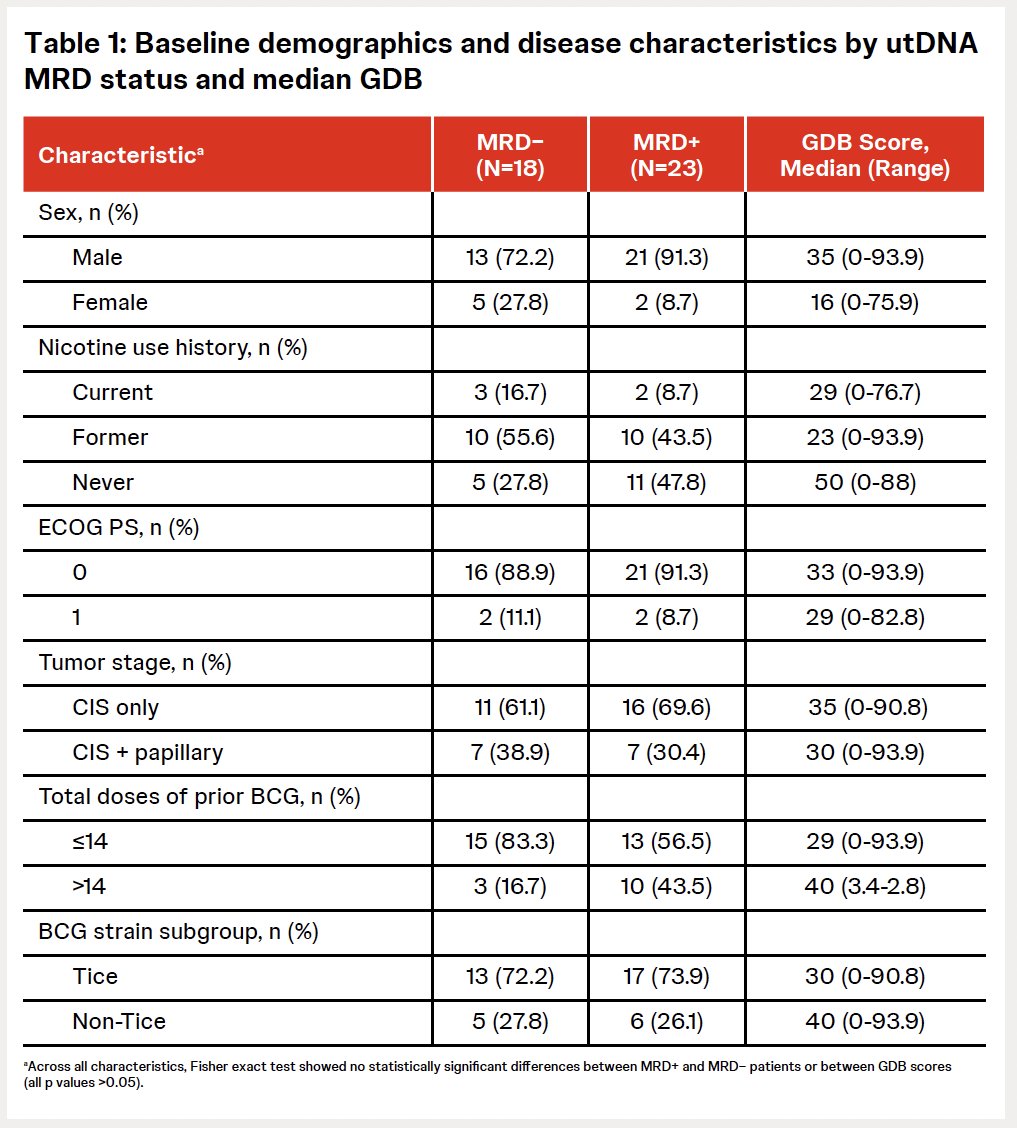
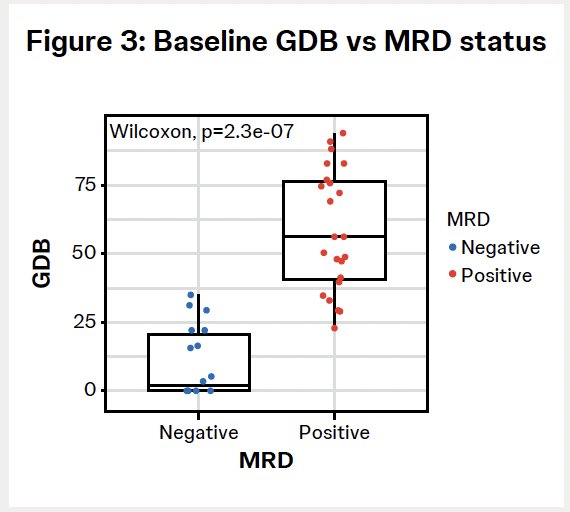
The baseline GDB scores were significantly different between MRD+ vs MRD- patients. The mean (SD) GDB scores were 58.4 (22.1) in utDNA MRD+ patients and 10 (12.8) in MRD- patients.
Efficacy Outcomes by Baseline utDNA MRD Status and GDB Scores
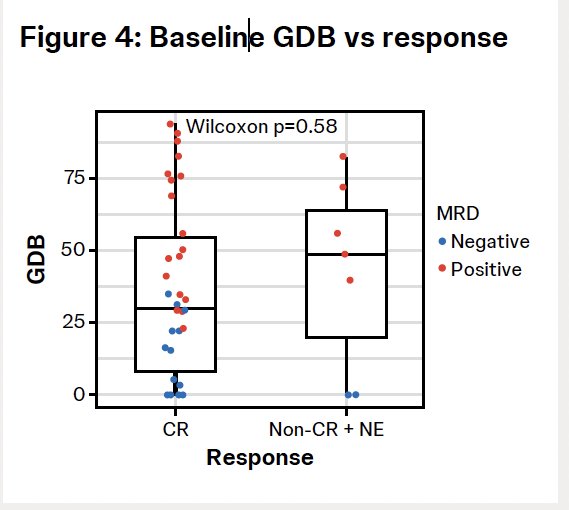
The CR rate was 78% (18/23) in patients who were utDNA MRD+ and 89% (16/18) in patients who were utDNA MRD- (p=0.44). The baseline GDB scores were not significantly different between patients with CR and those with non-CR or who were non-evaluable (mean: 36 versus 48.7). Baseline MRD status and GDB scores were not predictive of best overall response.
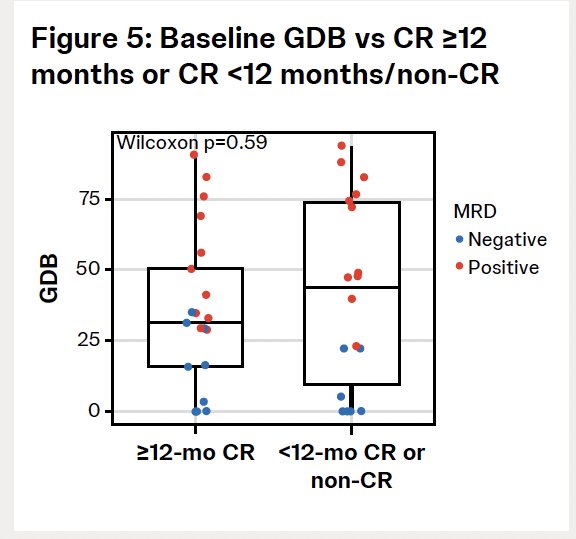
MRD status and GDB scores were similar between patients with CR ≥12 months versus those with CR <12 months or non-CR.
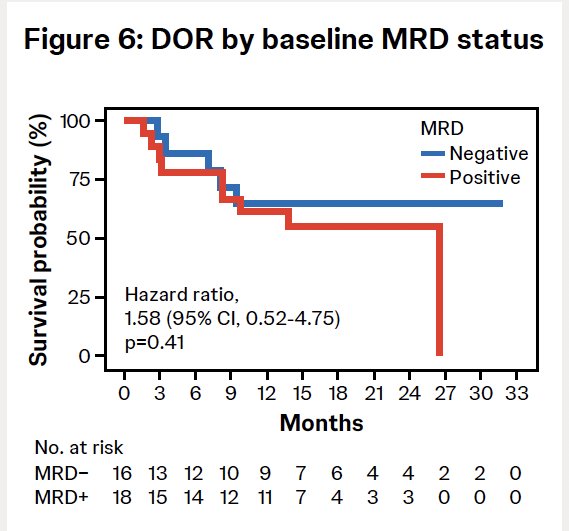
The 1-year duration of response was 61.1% (95% CI, 35.3-79.2) in utDNA MRD+ patients and 64.6% (95% CI, 34.7‑83.5) in utDNA MRD− patients.
Dr. Kulkarni concluded as follows:
- Baseline utDNA MRD status and genomic disease burden score were independent of patient demographics and tumor characteristics
- CR rate and durability of CR were consistent in subgroups of patients who were utDNA MRD+ or utDNA MRD- at baseline
- INLEXZO™ (previously TAR-200) monotherapy showed broad clinical activity in patients with BCG-unresponsive HR NMIBC with CIS independent of utDNA MRD status or GDB score
Presented by: Girish Kulkarni, MD, PhD, Professor, Department of Surgery, Division of Urology, University of Toronto, Toronto, ON, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
References
- Holzbeierlein JM, Smith A, Johnson B, et al. Outcomes of high-risk non–muscle invasive bladder cancer treated with intravesical BCG. J Urol. 2024;211(4):533-538.
- Lightfoot AJ, Breyer BN, Rosevear HM, et al. Recurrence and progression patterns in non–muscle invasive bladder cancer during long-term follow-up. Sci World J. 2011;11:602-613.
- American Urological Association; Society of Urologic Oncology. Diagnosis and treatment of non–muscle invasive bladder cancer: AUA/SUO guideline. Published 2020. Accessed 13 October 2025. https://www.auanet.org/guidelines-and-quality/guidelines/bladder-cancer-non-muscle-invasive-guideline
- Daneshmand S, Cookson MS, Kamat AM, et al. Gemcitabine intravesical drug-releasing system (TAR-200) for BCG-unresponsive CIS: Results from SunRISe-1. J Clin Oncol. 2025 Jul 30:JCO2501651. doi:10.1200/JCO-25-01651.
- Chauhan PS, Chen L, Varghese R, et al. Urinary tumor DNA for minimal residual disease detection in non–muscle invasive bladder cancer. PLoS Med. 2021;18(8):1-30.
- Narayan VM, Patel VG, Sfakianos JP, et al. Clinical utility of urinary tumor DNA in BCG-unresponsive bladder cancer. Eur Urol Oncol. 2025;8:425-434.
- Salari K, Chen J, Zhao S, et al. Genomic profiling of urinary tumor DNA in bladder cancer. Clin Cancer Res. 2023;29(18):3668-3680.