(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany was host to a urothelial carcinoma poster session. Dr. Felix Guerrero-Ramos presented the results of an exploratory analysis of the phase 2b SunRISe-1 trial in patients with BCG-unresponsive non-muscle invasive bladder cancer (NMIBC) with carcinoma in situ (CIS) +/- papillary disease, evaluating the association of molecular markers with clinical response to TAR-200.
TAR-200 is a novel intravesical drug-releasing system designed to provide sustained, localized delivery of gemcitabine within the bladder.1 TAR-200 has received the Breakthrough Therapy designation from the United States Food and Drug Administration in 2023 for treating high-risk NMIBC that is unresponsive to Bacillus Calmette-Guérin (BCG) and for which radical cystectomy (RC) is not an option.1-4 TAR-200 is currently being evaluated in the Phase 2b SunRISe-1 study (Cohort 2; Figure 1), involving patients with BCG-unresponsive HR-NMIBC with carcinoma in situ (CIS), with or without papillary tumors, who have declined or are ineligible for RC.5 The primary analysis results showed a complete response (CR) rate of 82.4% in Cohort 2, supporting TAR-200’s potential as an effective bladder-sparing therapy.5
Despite promising clinical efficacy of TAR-200, the biological factors influencing response remain unclear, highlighting the need to explore molecular and immune correlates to better understand treatment outcomes and guide future therapeutic strategies. The study objective was to evaluate the association between baseline molecular and immune biomarkers (including genomic alterations, programmed death-ligand 1 [PD-L1] expression, tumor mutational burden [TMB], microsatellite instability [MSI], and urine tumor DNA [utDNA] minimal residual disease [MRD]) and clinical response to TAR-200 monotherapy in patients with BCG-unresponsive HR-NMIBC (Cohort 2 of SunRISe-1 study).
The SunRISe-1 study design is illustrated below with Cohort 2, which received TAR-200 monotherapy, highlighted in red.

Tumor tissue genomic sequencing was performed as follows:
- Baseline tumor tissue samples were collected via transurethral resection of bladder tumor during screening. Genomic data were available for 44 baseline tissue samples from Cohort 2.
- Genomic profiling was performed using the TruSight Oncology 500 (TSO-500) panel (Omniseq Inc., USA).
Urine-based genomic profiling was performed as follows:
- Pre-treatment residual urine cytology pellets were submitted to Convergent Genomics (USA), where genomic profiling was conducted using the UroAmp assay, which evaluates 60 bladder cancer-related genes and detects MRD.
- Genomic data were available for 41 baseline urine samples.
In total, DNA profiles from 63 baseline samples (tissue or urine) were available. PD-L1 expression was assessed using the 22C3 clone via immunohistochemistry at LabCorp CLS, Los Angeles, and PD-L1 positivity was defined as a combined positive score ≥1. The molecular data from tissue and urine samples were correlated with complete response (CR; primary endpoint) and duration of response (DOR; secondary endpoint).
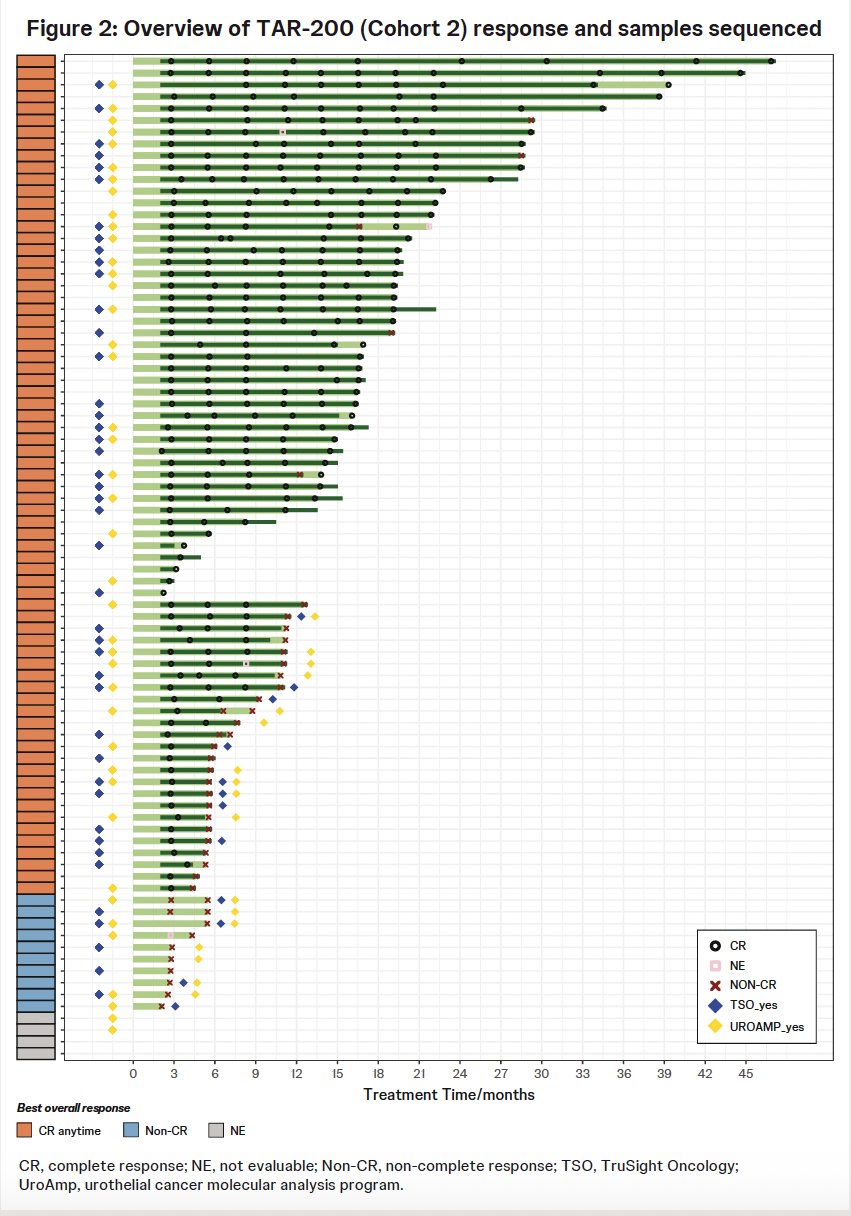
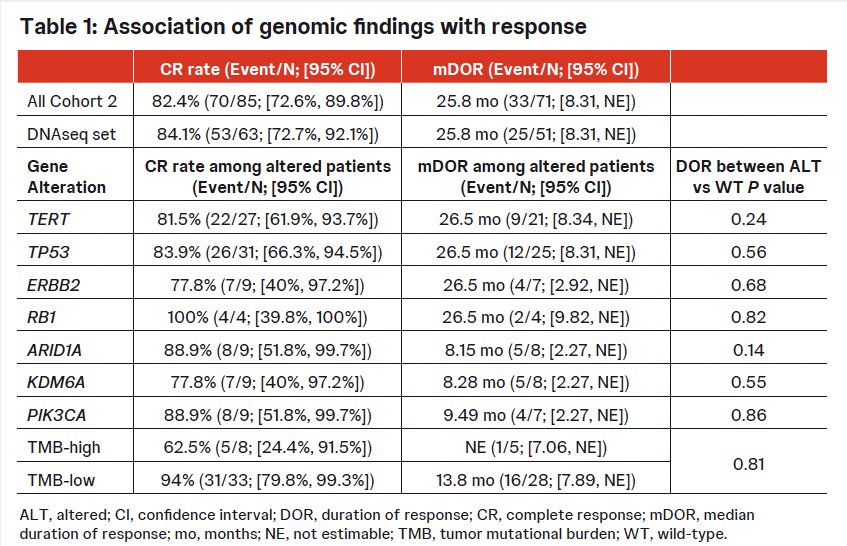
In Cohort 2, the CR rate was 82.4%, and the median DOR was 25.8 months. Among patients with available DNA sequencing data (n=63), the CR rate was 84% and the median DOR was 25.8 months.
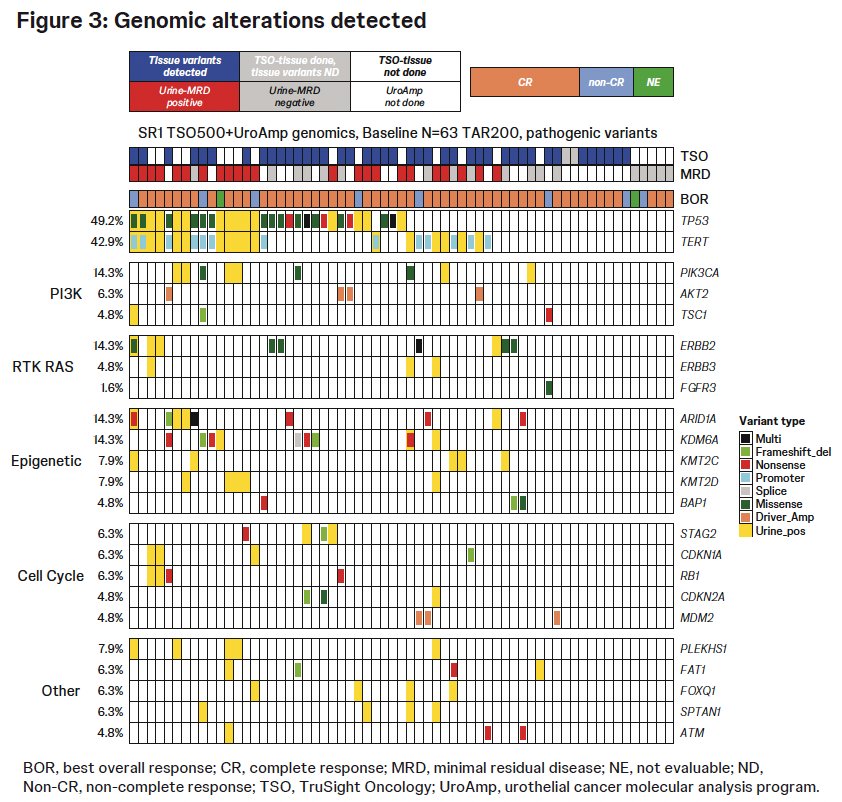
Genomic alterations were identified in 86% of tumors. The most frequently altered genes included:
– TP53: 49%
– TERT: 43%
– ERBB2: 14.3%
– PIK3CA: 14.3%
All evaluable tumors (n=41) were microsatellite stable. High TMB (>10 mutations/megabase) was observed in 19.5% of tumors.
No statistically significant differences in CR or DOR were observed between the genomic subgroups (all P>0.05; Table 1). Among TMB-high tumors, the CR rate was 63%, and the median DOR was not estimable.
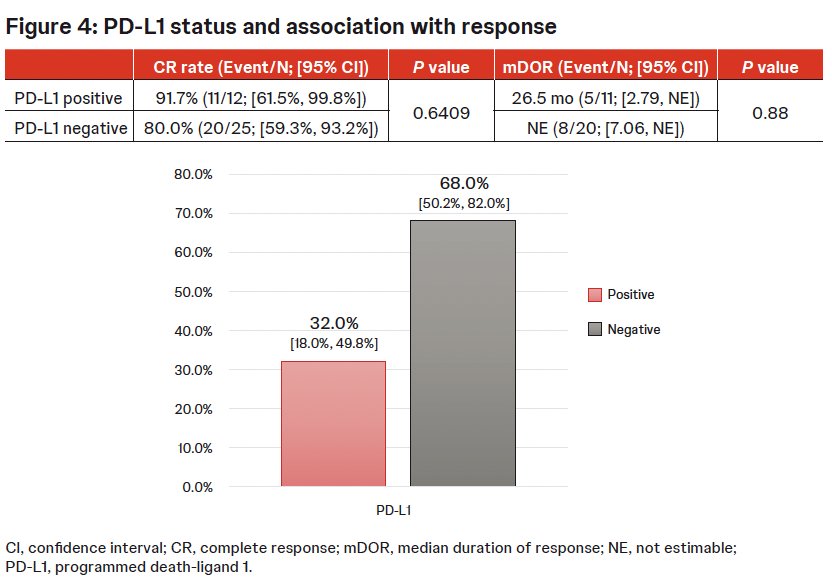
Of 37 patients tested for PD-L1 expression, 12 (32%) were PD-L1 positive. No statistically significant differences in CR or median DOR were observed between PD-L1 positive and negative groups.
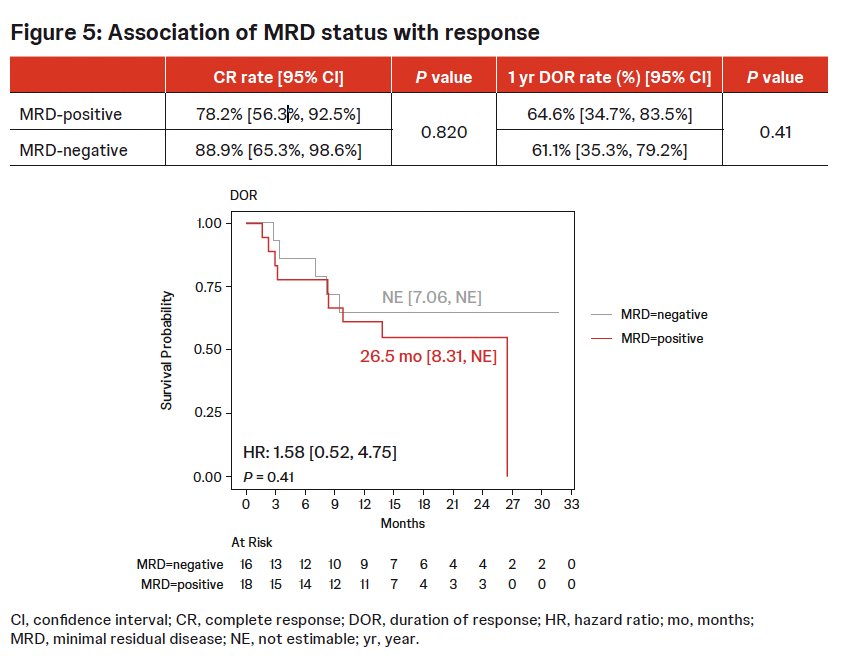
Among patients with available utDNA MRD data (n=41), MRD-positive patients (n=23) demonstrated a CR rate of 78% and a 1-year DOR rate of 65%. In comparison, MRD-negative patients (n=18) had a CR rate of 89% and a 1-year DOR rate of 61%. The median DOR was 26.5 months for MRD-positive patients and NE for MRD-negative patients. No statistically significant differences were observed in CR or median DOR between the two groups.
Dr. Guerrero-Ramos concluded as follows:
- Genomic alterations, PD-L1 expression, TMB, microsatellite stability, and utDNA MRD status did not significantly influence CR or DOR to TAR-200.
- The treatment showed consistent efficacy across molecular subgroups, supporting its potential as a bladder-sparing option for patients with BCG-unresponsive HR-NMIBC with CIS, with or without papillary tumors, ineligible for or refusing RC.
- These findings underscore the need for further research into predictive biomarkers to optimize patient selection and enhance therapeutic outcomes.
Presented by: Felix Guerrero-Ramos, MD, PhD, FEBU, Department of Urology, Hospital Universitario 12 de Octubre, Madrid, Spain
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: Biomarker Analysis from the SunRISe-1 Trial in BCG-Unresponsive CIS - Félix Guerrero-Ramos
References:
- Daneshmand S, Bazargani ST, Wang J, et al. Neoadjuvant pembrolizumab and enfortumab vedotin in cisplatin-ineligible patients with muscle-invasive bladder cancer: a multicenter phase II trial. Urol Oncol. 2022; 40(7):344.e1–344.e9.
- Tyson MD, Meeks JJ, Lobo N, et al. Pathologic response and survival outcomes with neoadjuvant gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin for muscle-invasive bladder cancer. J Urol. 2023;209(5):890–900.
- van Valenberg FJP, Tilki D, Seiler R, et al. Pathological complete response following neoadjuvant immune checkpoint inhibitors for muscle-invasive bladder cancer: a systematic review and meta-analysis. Eur Urol Open Sci. 2024;62:8–15.
- Daneshmand S, Pal SK, Galsky MD, et al. Neoadjuvant enfortumab vedotin plus pembrolizumab in cisplatin-eligible and cisplatin-ineligible patients with muscle-invasive bladder cancer: a multicentre, open-label, phase II trial. Urol Oncol. 2025;43(5):286–296.
- Daneshmand S, Galsky MD, Pal SK, et al. Neoadjuvant enfortumab vedotin plus pembrolizumab for muscle-invasive bladder cancer: results from the phase III VOLGA trial. J Clin Oncol. 2025;JCO2501651.