(UroToday.com) The 2025 South Central AUA annual meeting included a session on bladder cancer, featuring a presentation from Dr. Yair Lotan discussing 1-year outcomes of TAR-200 monotherapy in patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer CIS. Patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer have a high risk of disease progression and limited treatment options.
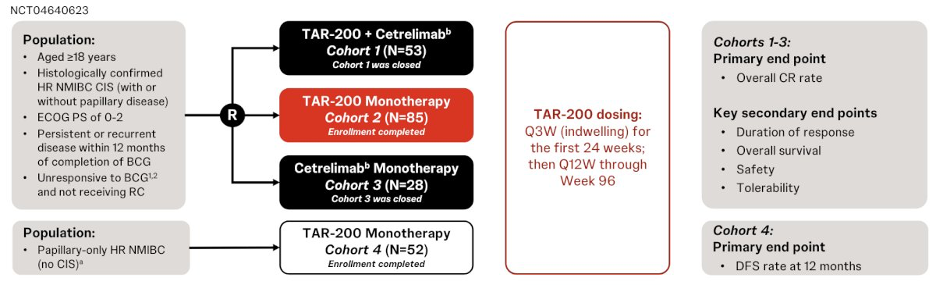
TAR-200 is an intravesical drug-releasing system designed to provide sustained delivery of gemcitabine in the bladder. SunRISe-1 (NCT04640623) is an ongoing phase 2b study assessing TAR-200 in patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer, ineligible for or refused radical cystectomy. Cohorts 1-3 enrolled patients with CIS ± papillary disease. At the 2025 South Central AUA annual meeting, Dr. Lotan and colleagues reported 1-year duration of response and patient-reported outcomes in patients receiving TAR-200 monotherapy (Cohort 2).
Dr. Lotan presented results from Cohort 2 of the SunRISe-1 trial, which included 85 patients who received TAR-200 every three weeks for the first 24 weeks, followed by administration every 12 weeks through week 96. The primary endpoint was the overall complete response rate, with key secondary endpoints including duration of response, overall survival, safety, tolerability, and health-related quality of life. Patients underwent quarterly cystoscopy, cytology, and mandated bladder biopsies at weeks 24 and 48. Patients who showed consistent disease progression while on treatment were required to be removed from the treatment arm:
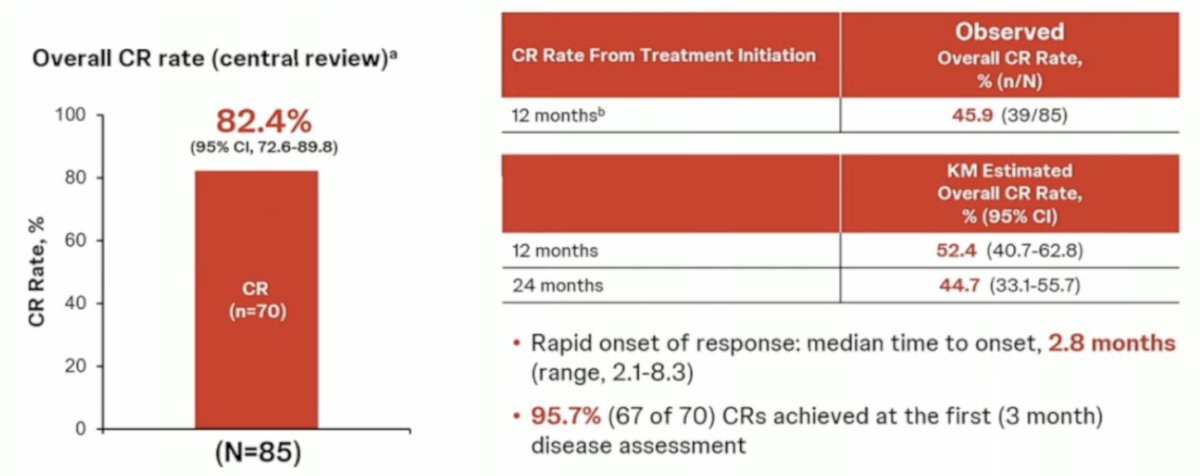
At the September 4, 2024 data cutoff, 85 patients (median age of 71 years [range: 40-88]; 80% male; 33% with concurrent papillary disease) received treatment, with a median follow-up of 14 months (range: 2-41). Cohort 2 demonstrated the highest complete response rate reported to date. The overall complete response rate was 82.4%, and the complete response rate from treatment initiation at 12 months was 45.9%. Responses occurred rapidly following TAR-200 monotherapy, with a median time to response of 2.8 months (range, 2.1–8.3 months). Notably, 95.7% (67 of 70) of complete responses were achieved by the first disease assessment at three months:
Of note, 52.9% of responses lasted for at least 12 months, and 47.1% of responses remain ongoing. Among the 11 patients who completed two years of treatment, nine patients continued to maintain their response. Durable responses were observed with TAR-200 monotherapy, with an estimated 12-month duration of response rate of 56.2%, and a median duration of response of 25.8 months. Additionally, 86.6% of patients remained cystectomy-free at one year: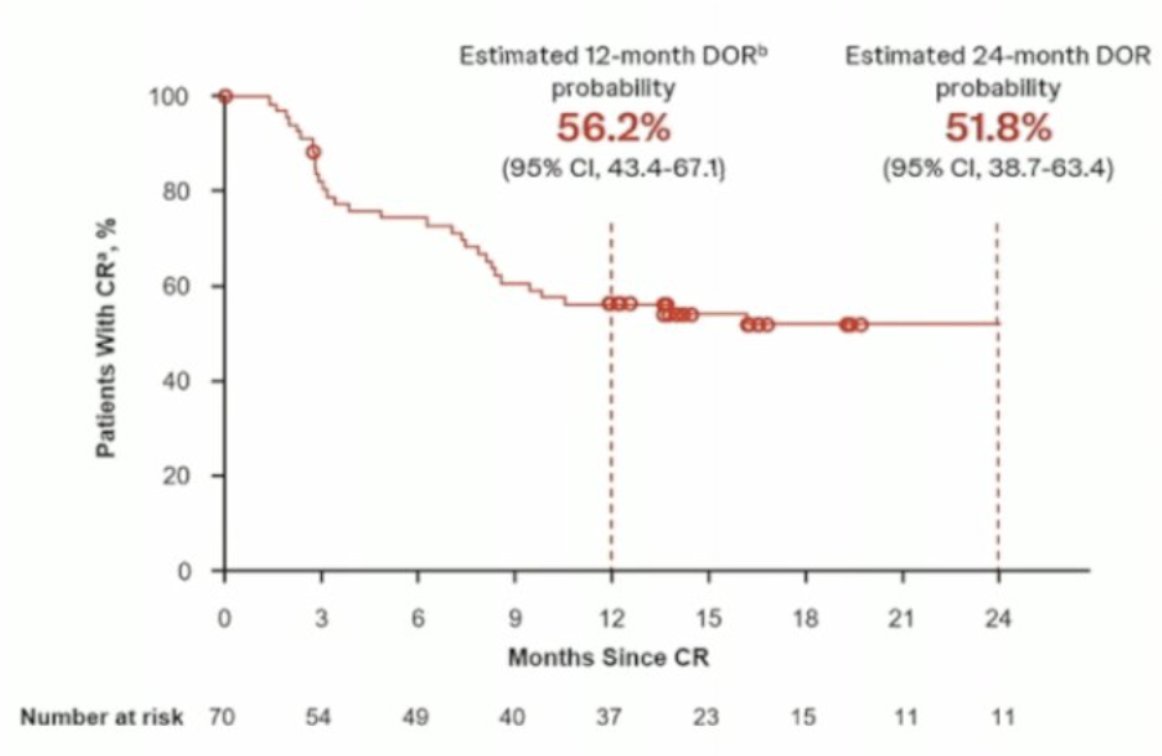
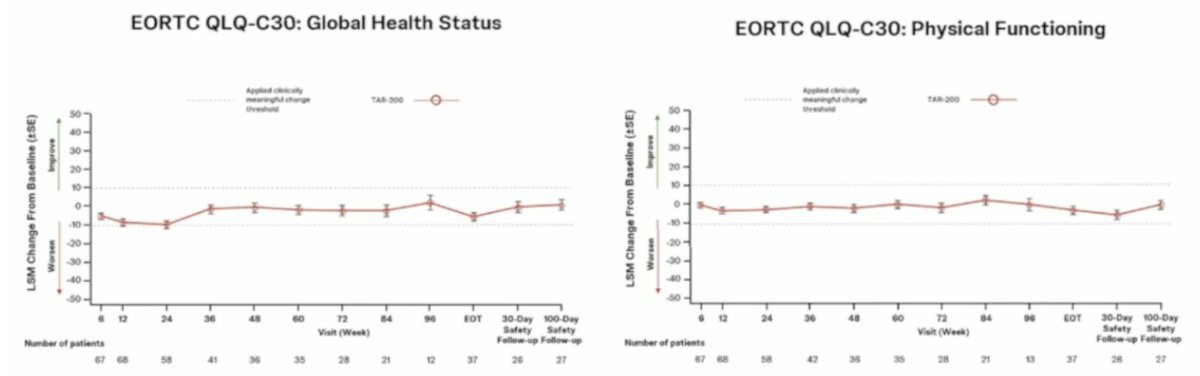
Patients maintained a stable quality of life while on TAR-200 treatment, with a mean EORTC QLQ-C30 Global Health Status score of 75.0 (SD 16.7) and physical functioning scores of 86.2 (SD 17.3) at baseline, and both remained stable throughout treatment:
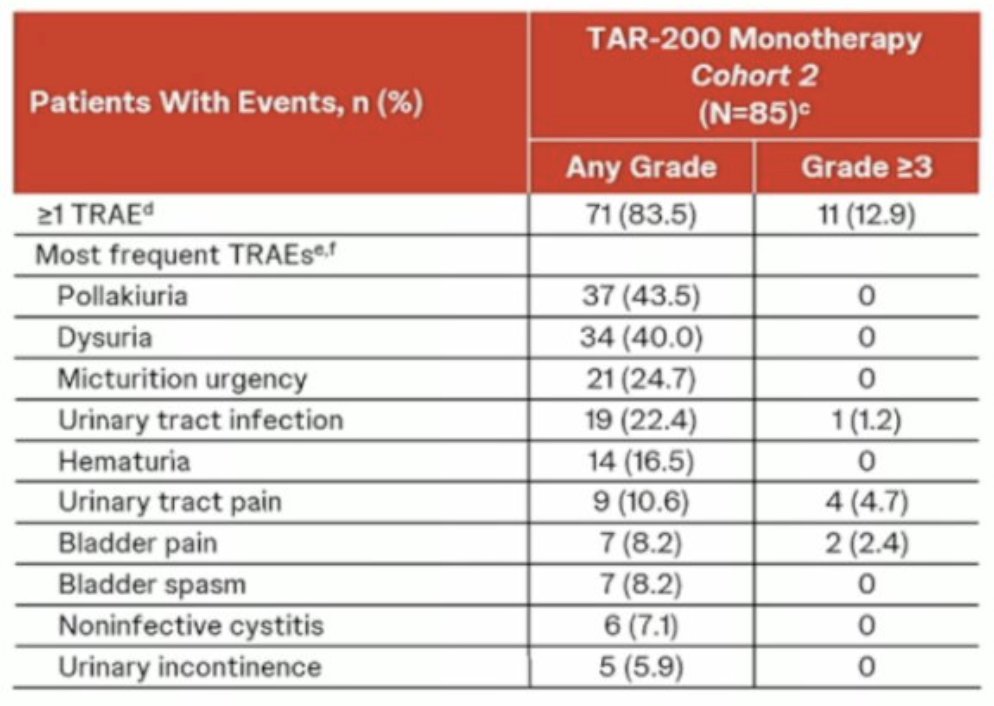
Most treatment-emergent adverse events were grade 1 or 2 (lower urinary tract adverse events) and resolved after a median of 3.1 weeks. Moreover, there was a 99% insertion success rate, with urologists reporting no significant difficulties placing the devices. Serious treatment-related adverse events occurred in 5 patients (5.9%), and only 3 patients (3.5%) discontinued treatment due to treatment-related adverse events. No treatment-related deaths were reported:
Dr. Lotan concluded his presentation discussing 1-year outcomes of TAR-200 monotherapy in patients with BCG-unresponsive high-risk NMIBC in situ with the following take-home points:
- TAR-200 monotherapy was well tolerated, with the highest complete response rate reported in BCG-unresponsive high-risk non-muscle invasive bladder cancer
- Responses were highly durable, and most responders were disease-free at 1 year
- Clinical benefit of TAR-200 was achieved with sustained overall health status and high physical function
- Based on these results, on September 9, 2025, TAR-200 monotherapy received FDA approval for BCG-unresponsive non-muscle invasive disease with CIS
Presented by: Yair Lotan, MD, Urologic Oncologist, UT Southwestern Medical Center, Dallas, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.