(UroToday.com) On the second day of the American Society for Clinical Oncology (ASCO) Genitourinary Cancer Symposium 2022 in Trials in Progress Poster Session B, Dr. Van Der Heijden presented the rationale and design of the SunRISe-1 trial of TAR-200 plus cetrelimab, TAR-200 alone, or cetrelimab alone in patients with high-risk nonmuscle-invasive bladder cancer (NMIBC) unresponsive to Bacillus Calmette-Guérin (BCG).
Dr. Van Der Heijden highlighted that treatment options are limited for patients with high-risk non-muscle-invasive bladder cancer (HR-NMIBC) unresponsive to intravesical bacillus Calmette–Guérin (BCG). While radical cystectomy is the gold standard treatment for these patients, many patients are unwilling or ineligible to undergo radical cystectomy. Thus, there is a substantial unmet need, and many ongoing trials in this disease space.
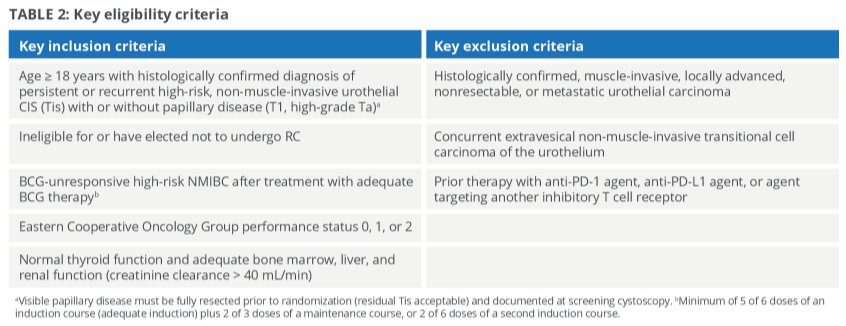
TAR-200 is an intravesical drug delivery system for local continuous release of gemcitabine within the bladder. The SunRISe-1 trial (NCT04640623) is an open-label, parallel-group, multicenter phase 2b study designed to assess the efficacy and safety of TAR-200 with cetrelimab, an anti–PD-1 antibody, TAR-200 alone, or cetrelimab alone in participants with BCG-unresponsive HR-NMIBC. To be eligible for inclusion, patients must be adults (age ≥ 18 years) with ECOG PS 0-2 and have recurrent or persistent histologically confirmed HR-NMIBC (carcinoma in situ) with or without papillary disease (T1, high-grade Ta) following BCG treatment (with less than 12 months elapsed from the last ECG treatment). Patients must be ineligible for or have declined radical cystectomy.
Following enrollment, approximately 200 patients will be randomized in a 2:1:1 fashion to receive TAR-200 + cetrelimab (Cohort 1, approximate n=100), TAR-200 (Cohort 2, approximate n=50), or cetrelimab (Cohort 3, approximate n=50).
In Cohorts 1 and 2, participants receive intravesical TAR-200 placed cystoscopically every 3 weeks through Week 24, and every 12 weeks thereafter until Week 96. In Cohorts 1 and 3, participants receive CET until Week 78. Primary disease assessments including cystoscopy, urine cytology, transurethral resection of bladder tumor [TURBT], and magnetic resonance imaging/computed tomography are performed initially at baseline. Subsequent cystoscopy and centrally read urine cytology are performed every 12 weeks through Year 2, every 24 weeks until end of Year 3, and in Year 4 and Year 5 in accordance with institutional standards of care. Further, TURBT is performed at 24 and 48 weeks. Additionally, patients will undergo axial imaging with CT or MRI with contrast every 24 weeks through Year 3.
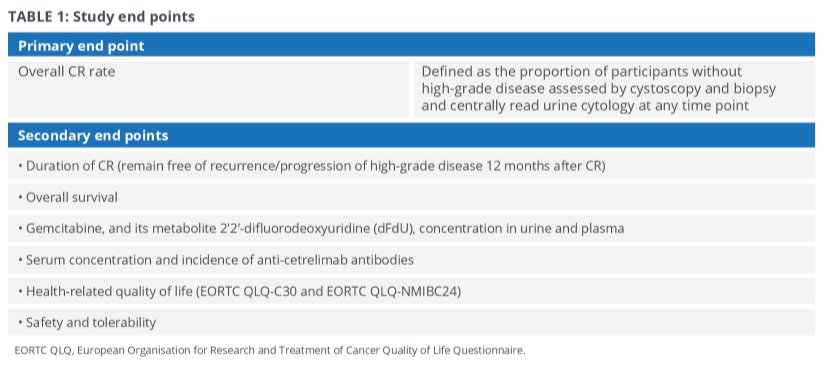
The primary endpoint for all three cohorts is overall CR rate at any time point. Additionally, secondary endpoints include duration of response (ie, from time of first CR achieved to first evidence of recurrence, progression, or death [whichever is earlier] for participants who achieve a CR), overall survival, PK immunogenicity of cetrelimab, safety and tolerability, and patient-reported outcomes.
Exploratory end points include incidence and time to cystectomy (measured from randomization to date of cystectomy), biomarkers, and health care resource utilization. This study opened in January 2021 and is enrolling participants at approximately165 study sites in 17 countries in North America, Europe, Asia, and Australia. The study is expected to reach primary completion on October 24, 2024.
Presented by: Michiel Simon Van Der Heijden MD, Ph.D., Netherlands Cancer Institute, Amsterdam, Netherlands