Dr. Suzanne Merrill reviewed recent updates in immunotherapy for bladder cancer, noting a strong biologic rationale for its use given the disease’s capacity to evade immune detection and destruction. Bladder cancer can downregulate tumor antigen presentation and inactivate cytotoxic T-cells, thereby creating an immunosuppressive microenvironment:
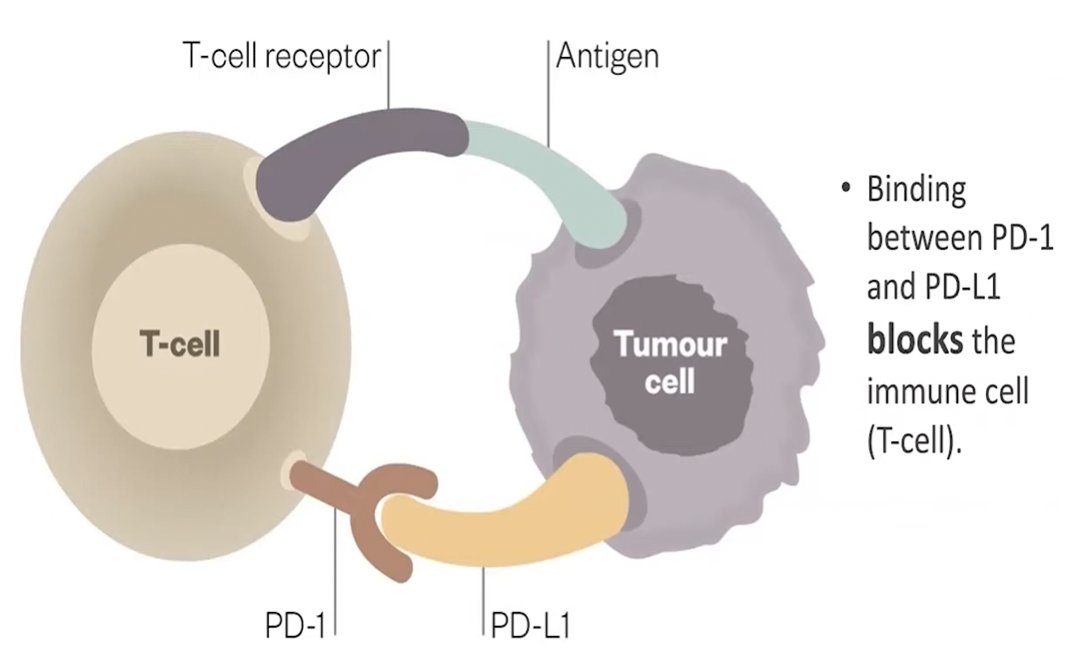
The role for immunotherapy is to reactivate and enhance the activity of CD8+ cytotoxic T-cells and production of natural killer effector cells, which leverages the body’s own immune system to recognize and attack:
Certainly, there are limitations of BCG monotherapy, providing a rationale for combining BCG with immune checkpoint inhibitors in non-muscle invasive bladder cancer. These limitations include:
- High-risk patients have a high recurrence rate (year 1 – 60%; year 5 – 78%) and a high risk of progression (30%)
- BCG has a high initial complete response, but poor durability
- The risk of becoming BCG unresponsive ranges from 30%-50%
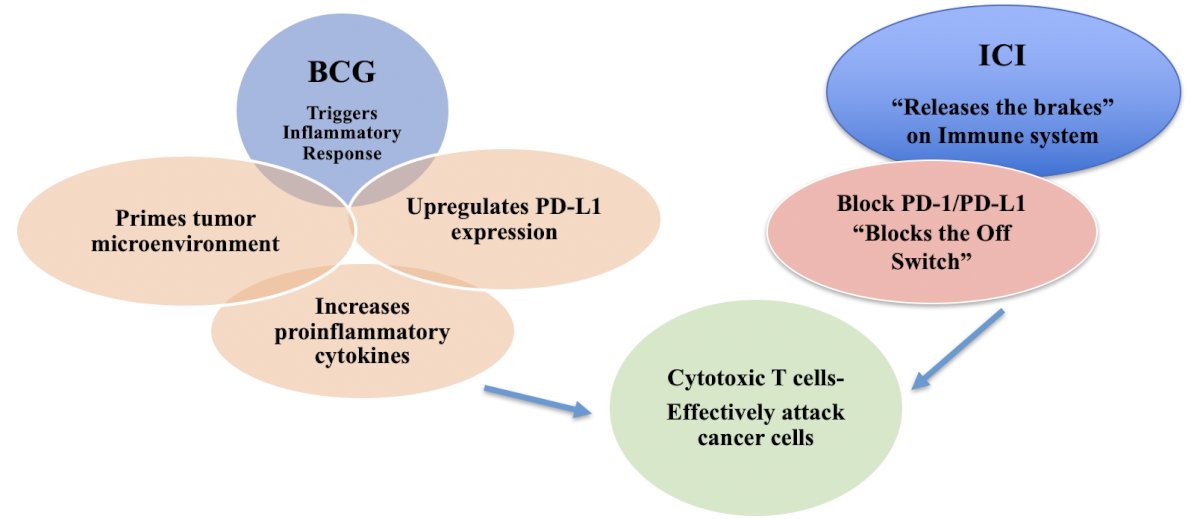
BCG primes the immune response and initiates a strong inflammatory response, which then recruits and activates immune cells that prime the tumor microenvironment, while immune checkpoint inhibitors then "release the brakes" on the immune system, allowing T cells to more effectively attack cancer cells:
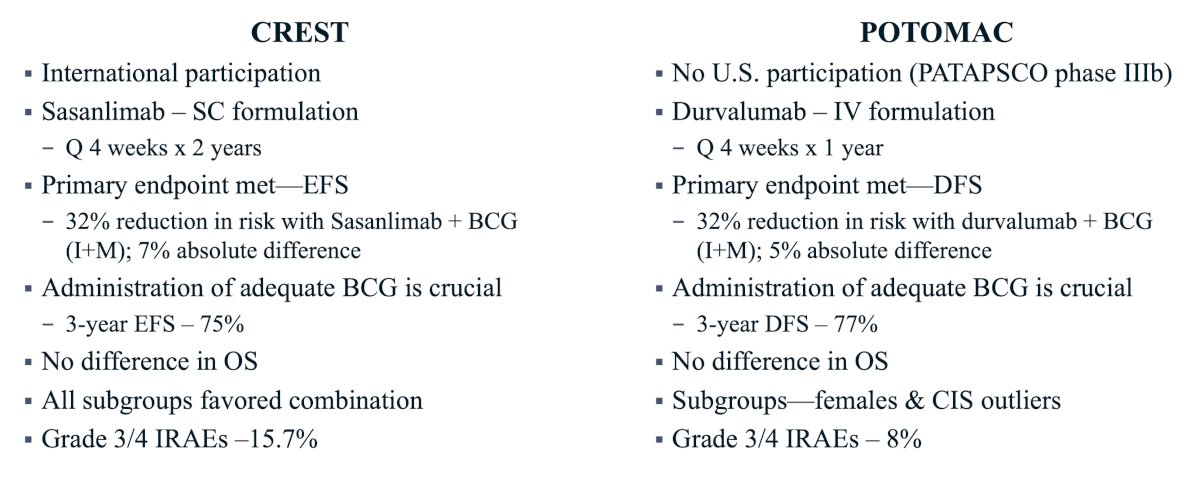
Dr. Merrill then discussed several of the new clinical trials in the BCG-naïve disease space. The CREST trial1 was presented at AUA 2025, which was a three-arm study comparing different combinations of sasanlimab and BCG. Arm A received sasanlimab administered subcutaneously combined with BCG (induction and maintenance), Arm B received sasanlimab with BCG (induction only), and Arm C received BCG (induction and maintenance) alone. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause: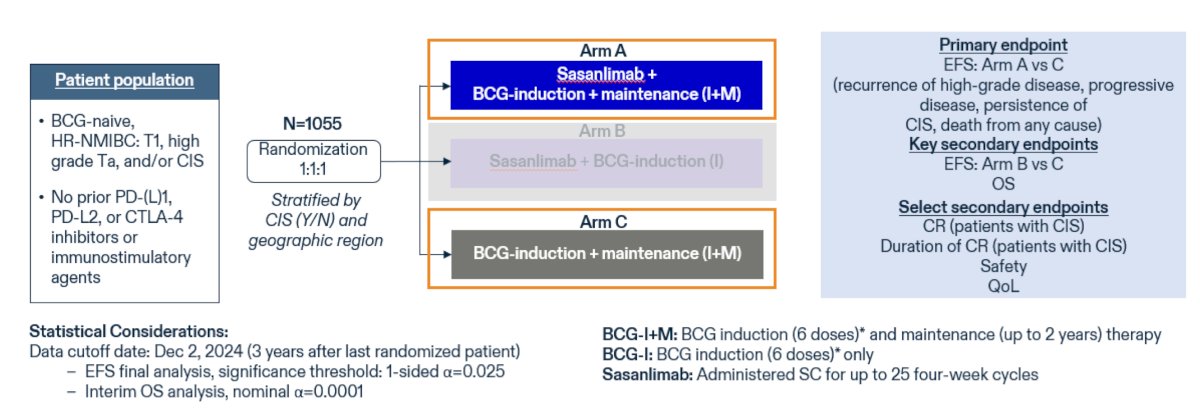
There were several key findings from the CREST trial:
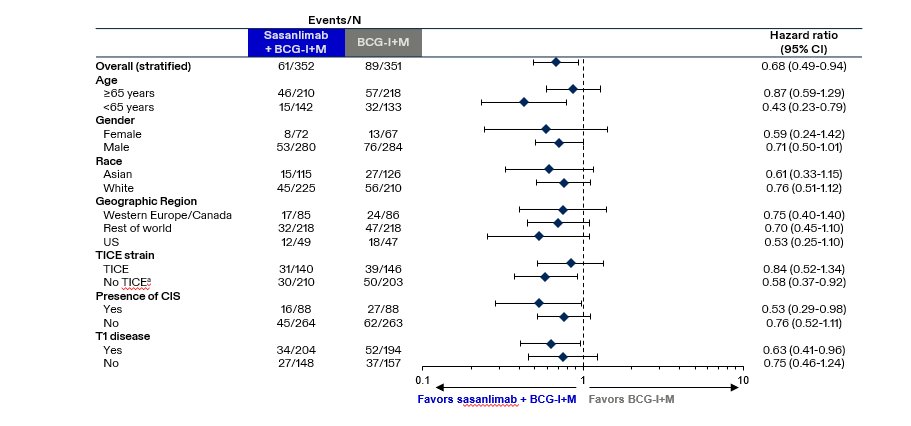
- The primary endpoint of event-free survival was met: 32% lower with sasanlimab + BCG (induction and maintenance) compared to BCG (induction and maintenance) alone (stratified HR 0.68, 95% CI 0.49–0.94; 1-sided p-value: 0.0095)
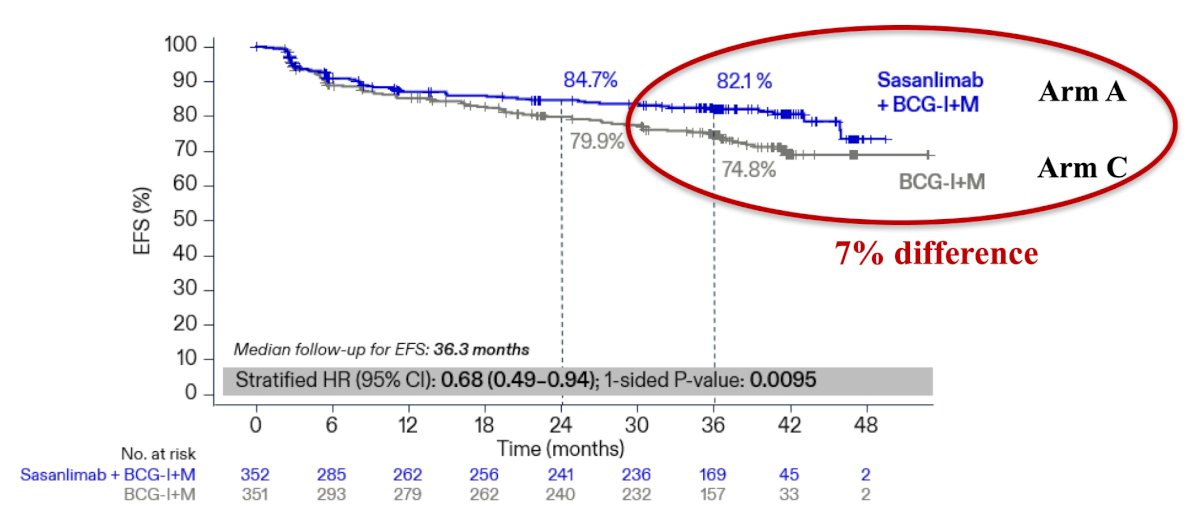
- Administration of adequate BCG is crucial: 3-year event-free survival was 75% in the BCG (induction and maintenance) alone arm
- All subgroups favored the sasanlimab + BCG combination:
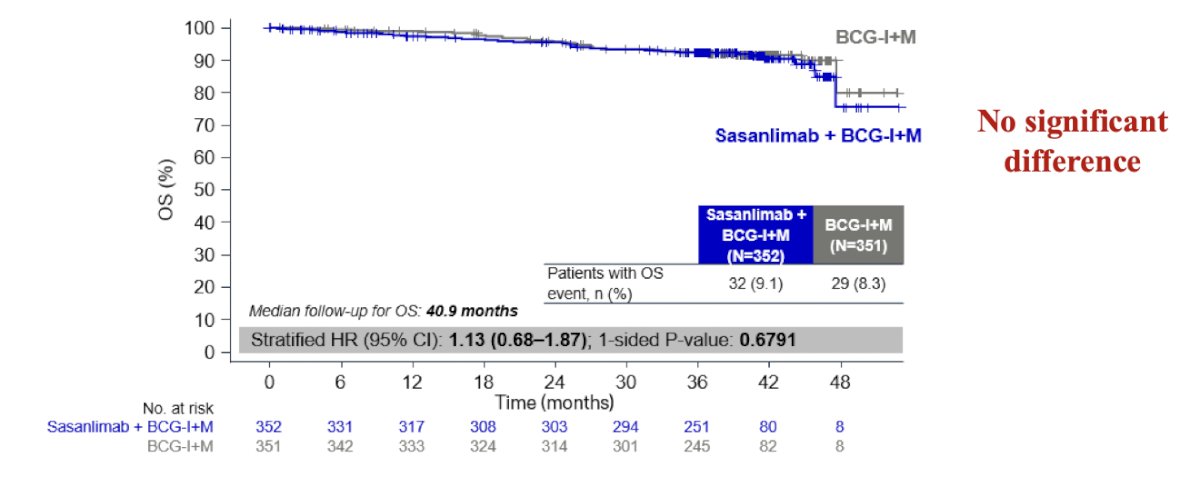
- There was no difference in overall survival:
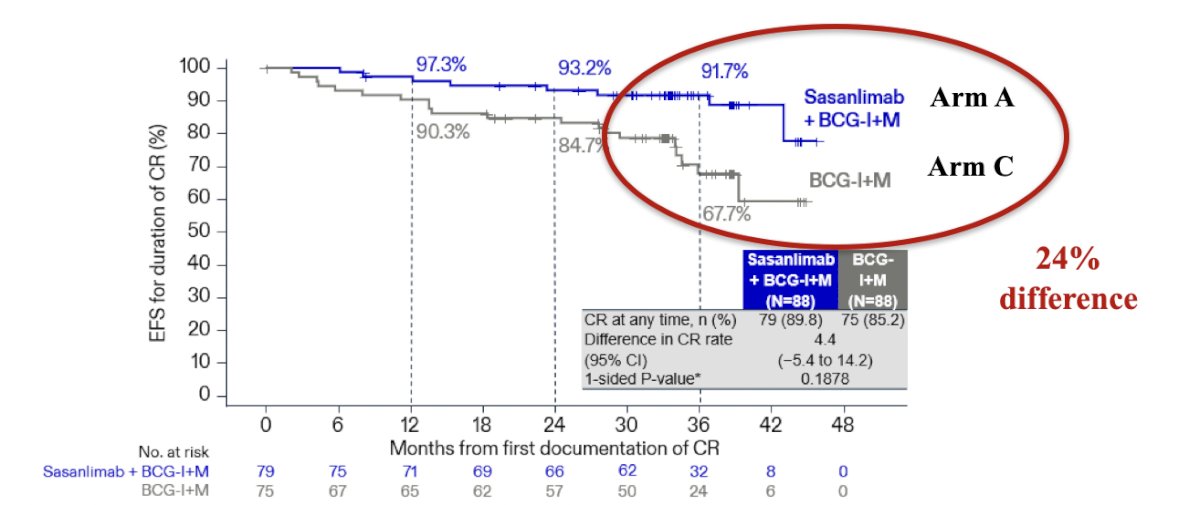
- In patients with CIS, the probability of maintaining a complete response at 36 months was 91.7% with sasanlimab + BCG (induction and maintenance), compared to 67.7% with BCG (induction and maintenance) alone:
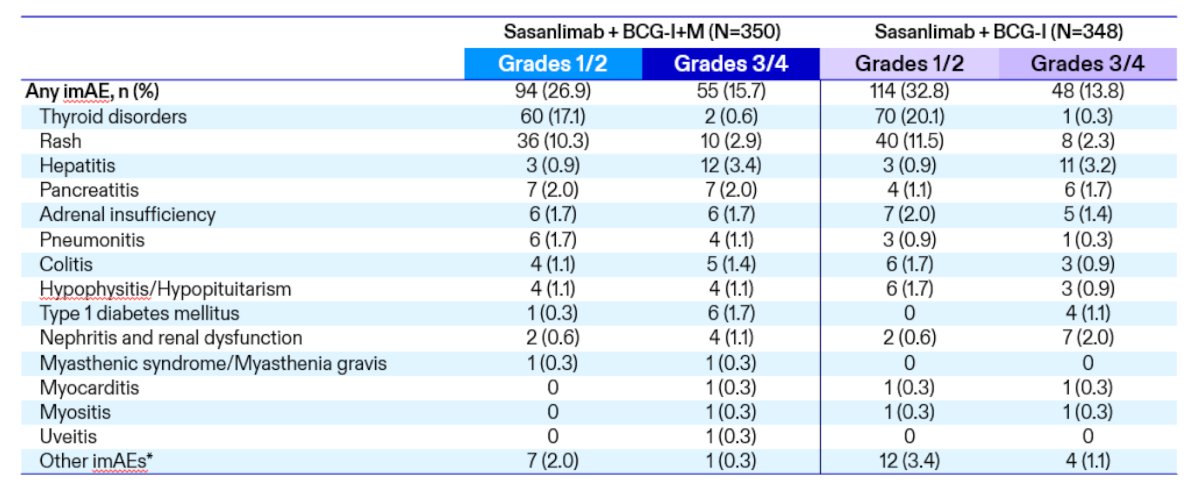
- The grade 3/4 immune-related adverse event rate was 15.7%
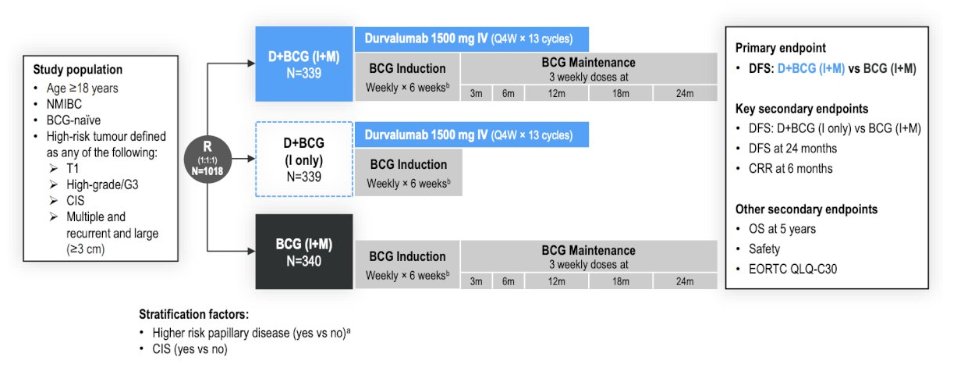
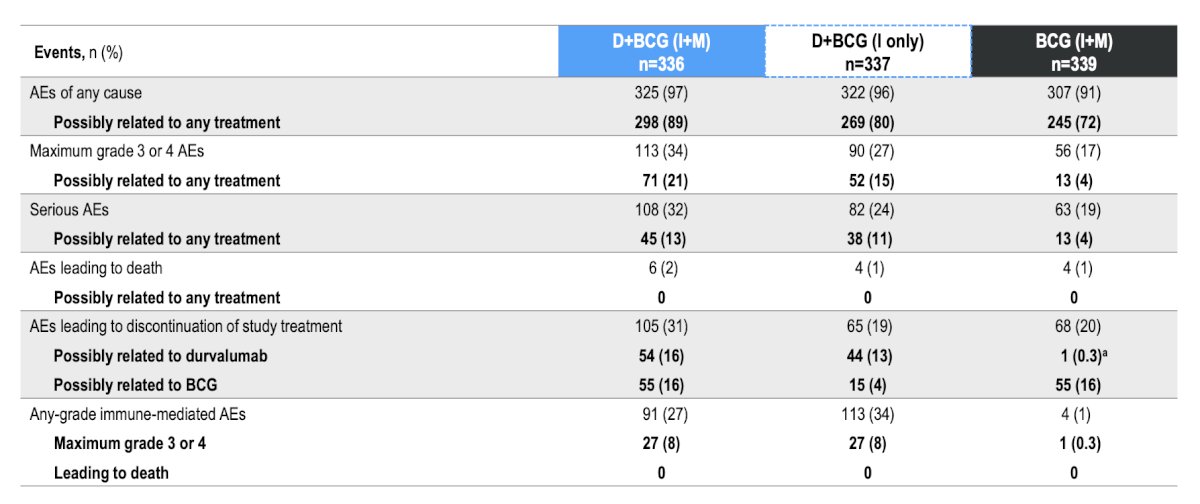
The next trial Dr. Merrill discussed was the POTOMAC trial,2 initially presented at ESMO 2025. In POTOMAC, eligible adult patients with BCG-naïve, local histologically confirmed high-risk non-muscle-invasive bladder cancer who had TURBT (complete resection, including patients with residual CIS) were randomized 1:1:1 to receive durvalumab + BCG (induction + maintenance), durvalumab + BCG induction only, or BCG (induction + maintenance). Durvalumab was administered intravenously (1500 mg every 4 weeks for 13 cycles), and intravesical BCG was given weekly × 6 weeks (induction only) and as 3 weekly doses at 3, 6, 12, 18, and 24 months. Patients were stratified by higher-risk papillary disease and CIS. The primary endpoint was investigator-assessed disease free survival with durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance):
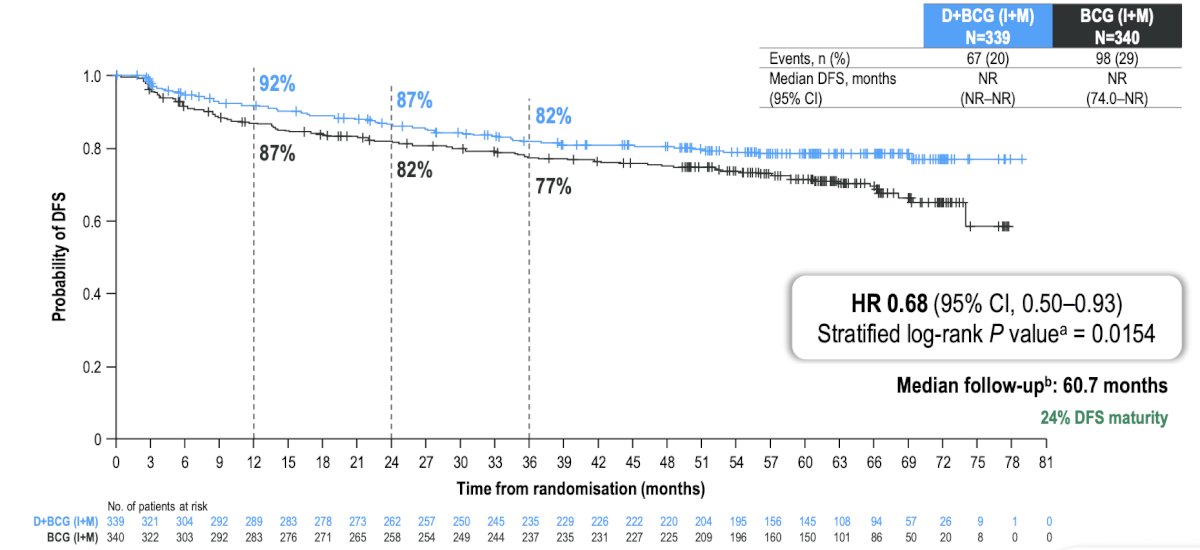
The median follow-up was 60.7 months. The primary endpoint of disease free survival was met with a 32% reduction in risk of recurrence of high-risk disease or death by any cause for durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) (HR 0.68, 95% CI 0.50–0.93; log-rank p = 0.0154), and 24-month disease free survival rates were 86.5% (95% CI 82.2–89.8) for durvalumab + BCG (induction + maintenance) and 81.6% (95% CI 76.9–85.3) for BCG (induction + maintenance):
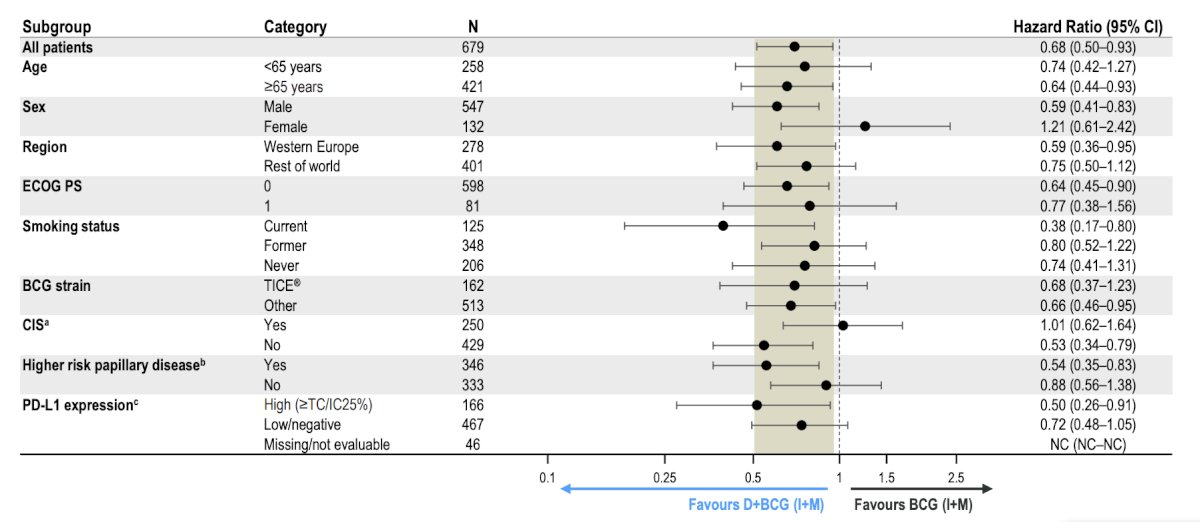
In the disease-free survival subgroup analyses, there was a generally consistent treatment effect across subgroups for durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) arms:
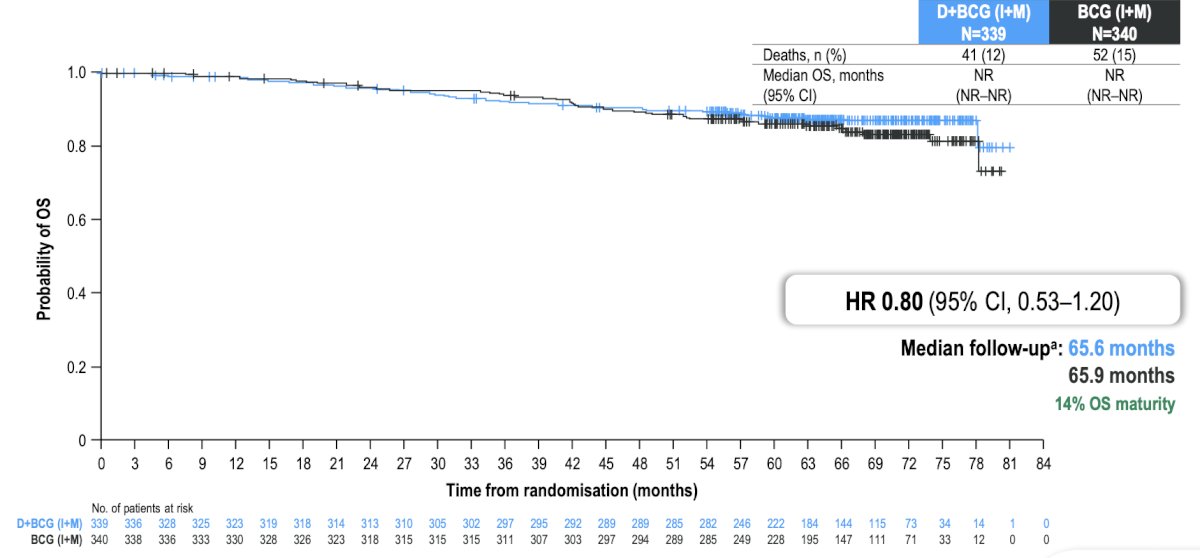
No evidence of overall survival detriment was seen with durvalumab + BCG (induction + maintenance) versus BCG (induction + maintenance) (descriptive analysis: HR 0.80, 95% CI 0.53–1.20):
Grade 3/4 treatment-related adverse events occurred in 21% of patients with durvalumab + BCG (induction + maintenance), in 15% with durvalumab + BCG (induction only), and in 4% with BCG (induction + maintenance). No treatment-related adverse events led to death:
Dr. Merrill noted the following key takeaways from the CREST and POTOMAC trials:
Ultimately, she notes that the decision we will have to contend with in the future, once these combination therapies are approved, is what specific subgroups of patients may benefit to where the disease benefit outweighs the toxicity risk. Ideally, biomarkers will help make this decision clearer.
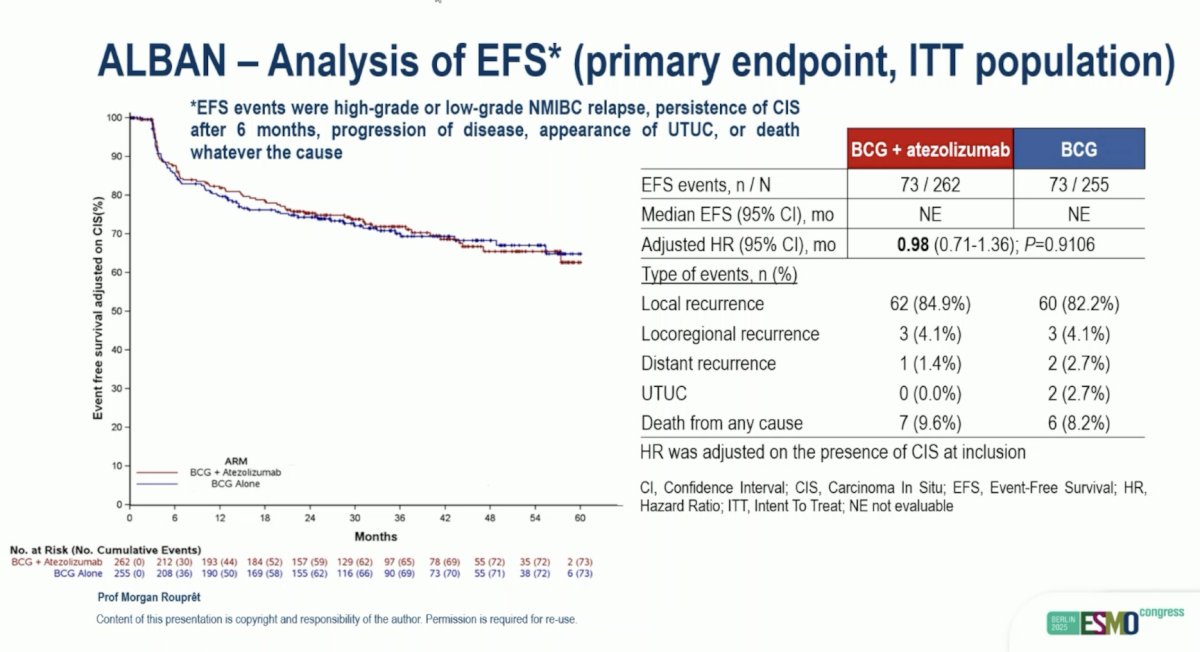
Next, Dr. Merrill discussed the ALBAN trial, initially presented at ESMO 2025. Eligible patients in ALBAN had histologically confirmed non muscle-invasive bladder cancer with high-risk features, no prior BCG therapy, ECOG performance status 0-2 were randomized 1:1 to BCG (6-weekly instillations followed by 3-weekly maintenance instillations at 3, 6, 12 months [Arm A]) or atezolizumab (1200 mg IV every 3 weeks for up to 1 year) combined with BCG delivered as in Arm A (Arm B). Randomization was stratified by the presence of CIS, and the primary endpoint was event-free survival. Key secondary endpoints included high-grade recurrence-free survival, overall survival, and safety. The trial design for ALBAN is as follows:
![Next, Dr. Merrill discussed the ALBAN trial, initially presented at ESMO 2025. Eligible patients in ALBAN had histologically confirmed non muscle-invasive bladder cancer with high-risk features, no prior BCG therapy, ECOG performance status 0-2 were randomized 1:1 to BCG (6-weekly instillations followed by 3-weekly maintenance instillations at 3, 6, 12 months [Arm A]) or atezolizumab (1200 mg IV every 3 weeks for up to 1 year) combined with BCG delivered as in Arm A (Arm B). Randomization was stratified by the presence of CIS, and the primary endpoint was event-free survival. Key secondary endpoints included high-grade recurrence-free survival, overall survival, and safety. The trial design for ALBAN is as follows:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-recent-updates-in-immunotherapy-in-bladder-cancer/image-15.jpg)
At the data cut-off date of January 9, 2025, the median follow-up was 35.3 months (range: 0-60). There was no statistically significant difference in event-free survival between arms (HR 0.98, 95% CI 0.71-1.36, p = 0.9106):
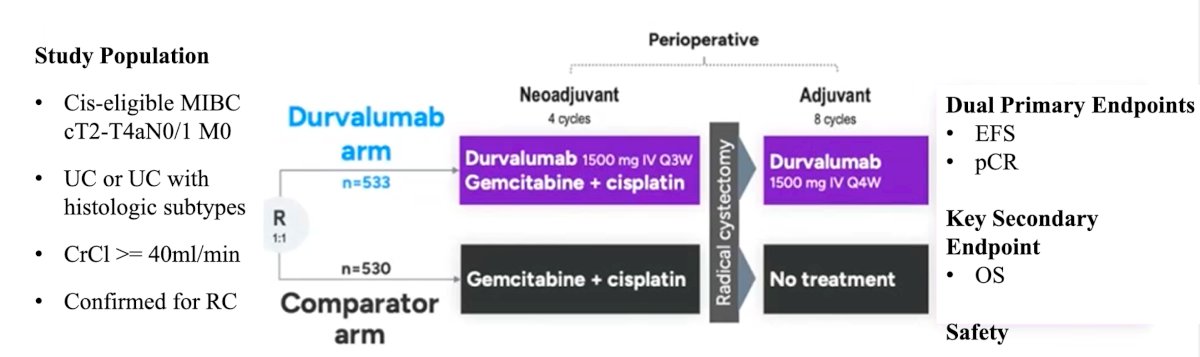
Recently, there has been a paradigm shift in muscle-invasive bladder cancer, given the new perioperative regimen assessed in the NIAGARA trial.4 NIAGARA was the first global phase 3 study to evaluate a perioperative immunotherapy, durvalumab, combined with neoadjuvant chemotherapy in cisplatin-eligible patients with muscle-invasive bladder cancer:1
There were several key findings from the CREST trial:
- The trial met the primary endpoint of improved event-free survival: 32% risk reduction at 24 months (durvalumab + gemcitabine + cisplatin 67.8% versus gemcitabine + cisplatin 59.8%)
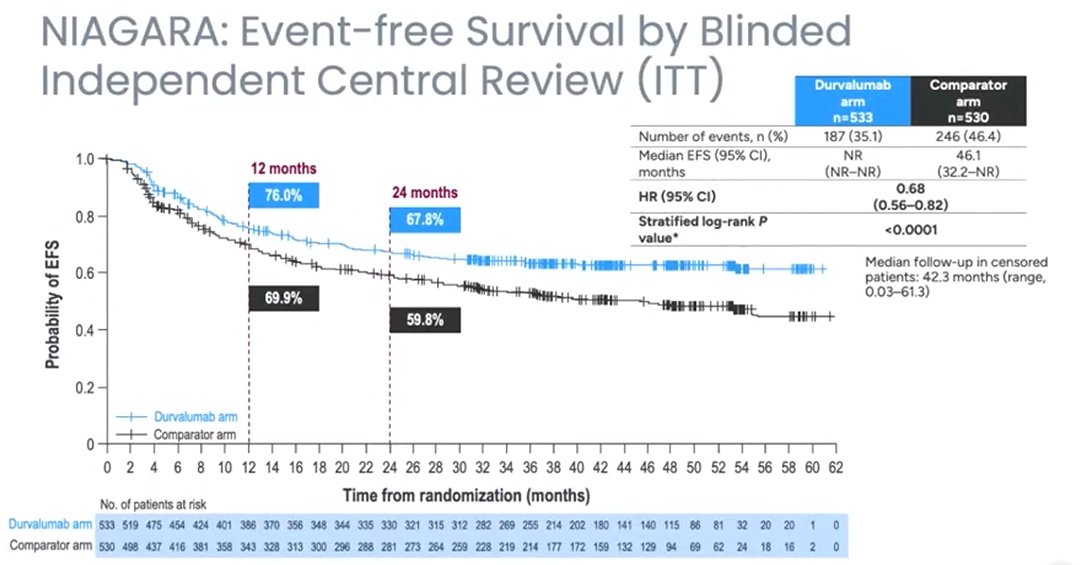
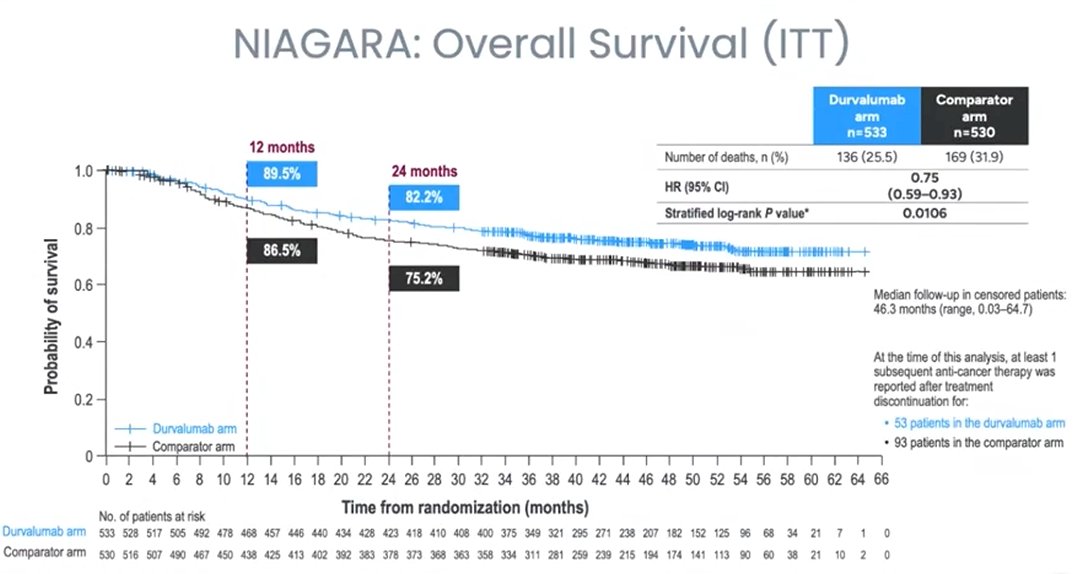
- The trial also met the key secondary endpoint of improved overall survival: 25% risk reduction at 24 months (durvalumab + gemcitabine + cisplatin 82.2% versus gemcitabine + cisplatin 75.2%). NIAGARA showed an overall survival benefit in the neoadjuvant setting, for the first time showing this benefit by adding a novel agent to the standard of care, and early in the study maturity
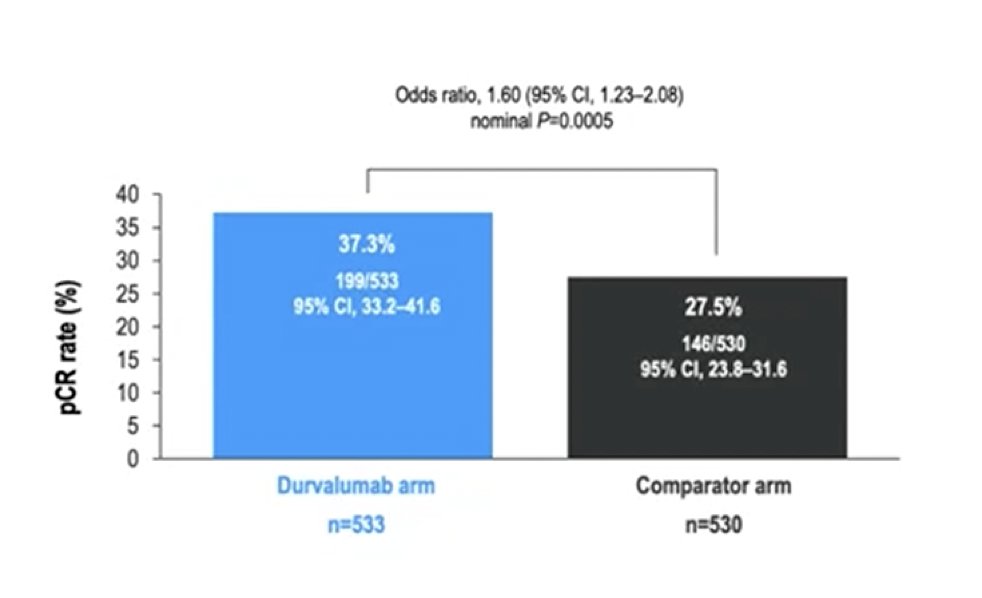
- Pathologic complete response was 10% higher with durvalumab: 37.5% versus 27.5%
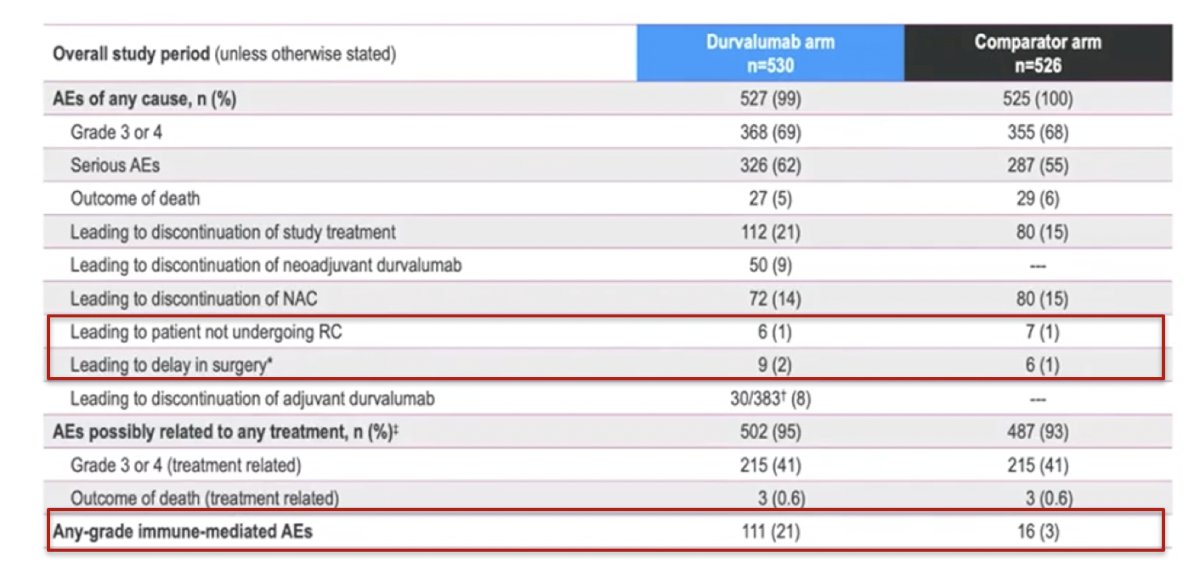
- Most grade 3/4 adverse events were driven by the cytotoxic component
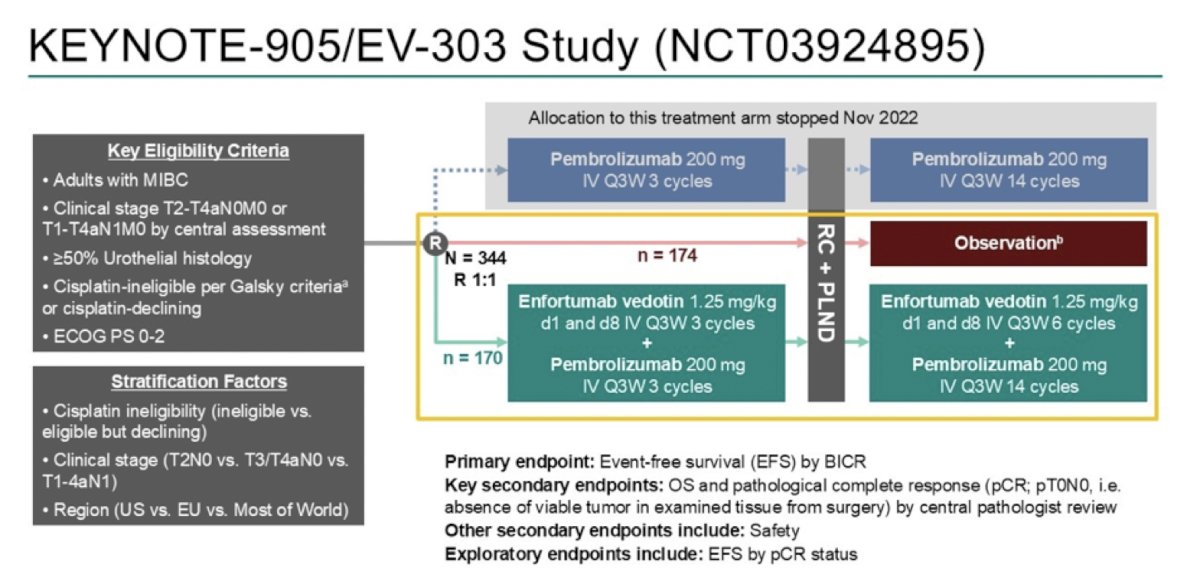
The KEYNOTE-905/EV-303 trial was first presented at ESMO 2025, enrolling adults with muscle-invasive bladder cancer (≥50% urothelial histology) who were either cisplatin ineligible per Galsky criteria or declined cisplatin, had an ECOG performance status of 0-2, and clinical stage T2-T4aN0M0 or T1-T4aN1M0 disease. Prior to radical cystectomy, patients were randomized across three study arms: (i) pembrolizumab IV every 3 weeks for 3 cycles, (ii) immediate radical cystectomy, or (iii) enfortumab vedotin IV every 3 weeks for 3 cycles + pembrolizumab IV every 3 weeks for 3 cycles:
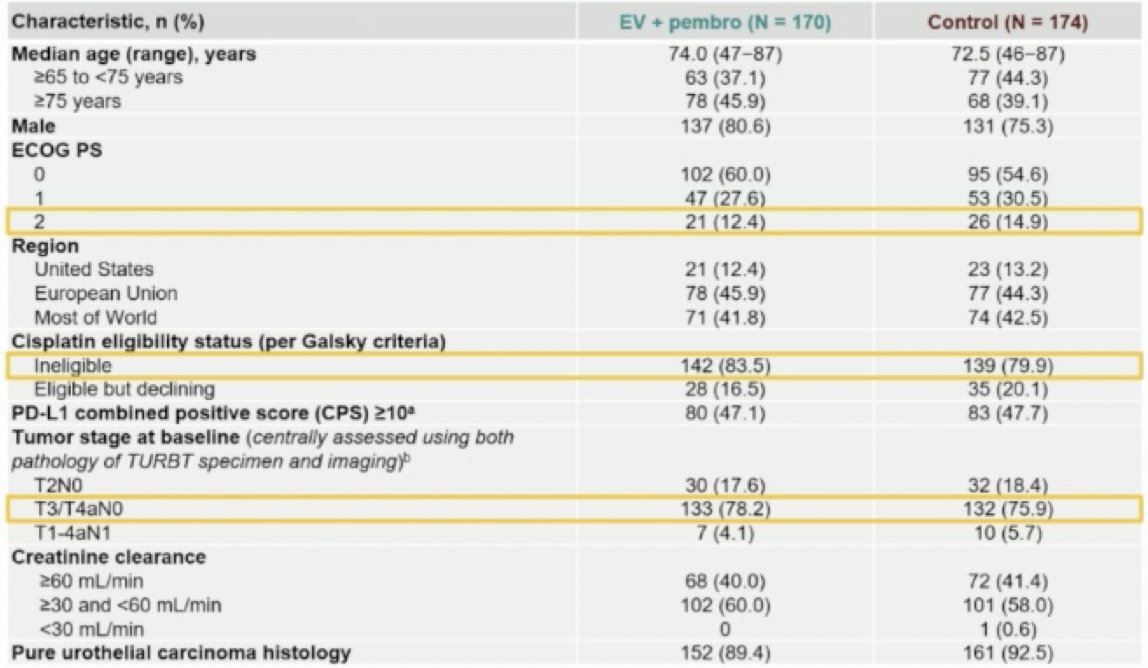
The median age was 74.0 years in the experimental arm and 72.5 years in the control arm, older than in prior muscle-invasive bladder cancer trials. By comparison, median ages were 63–66 years in cisplatin-eligible trials such as NIAGARA4 and VESPER,5 and 12-15% of patients were ECOG performance status 2. Approximately 80% were cisplatin-ineligible, most commonly due to renal impairment. Tumor stage was centrally assessed using both TURBT pathology and imaging, with most patients presenting T3/T4aN0 disease:
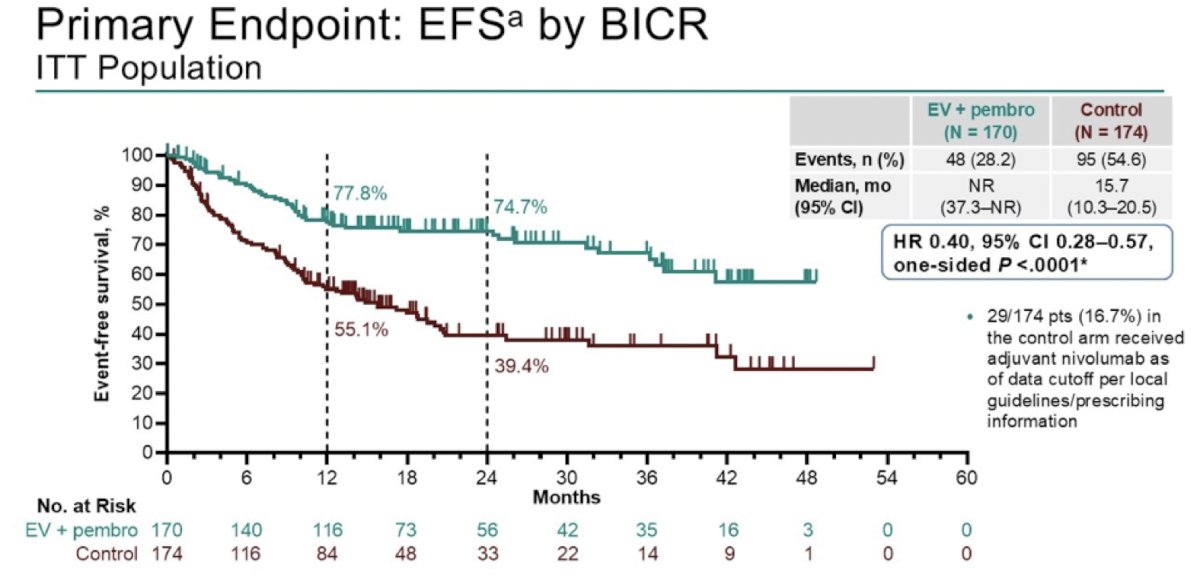
The primary endpoint of event-free survival by blinded independent central review demonstrated a significant improvement with enfortumab vedotin + pembrolizumab versus control, with median event-free survival not reached compared to 15.7 months (HR 0.40, 95% CI 0.28–0.57; one-sided p < 0.0001):
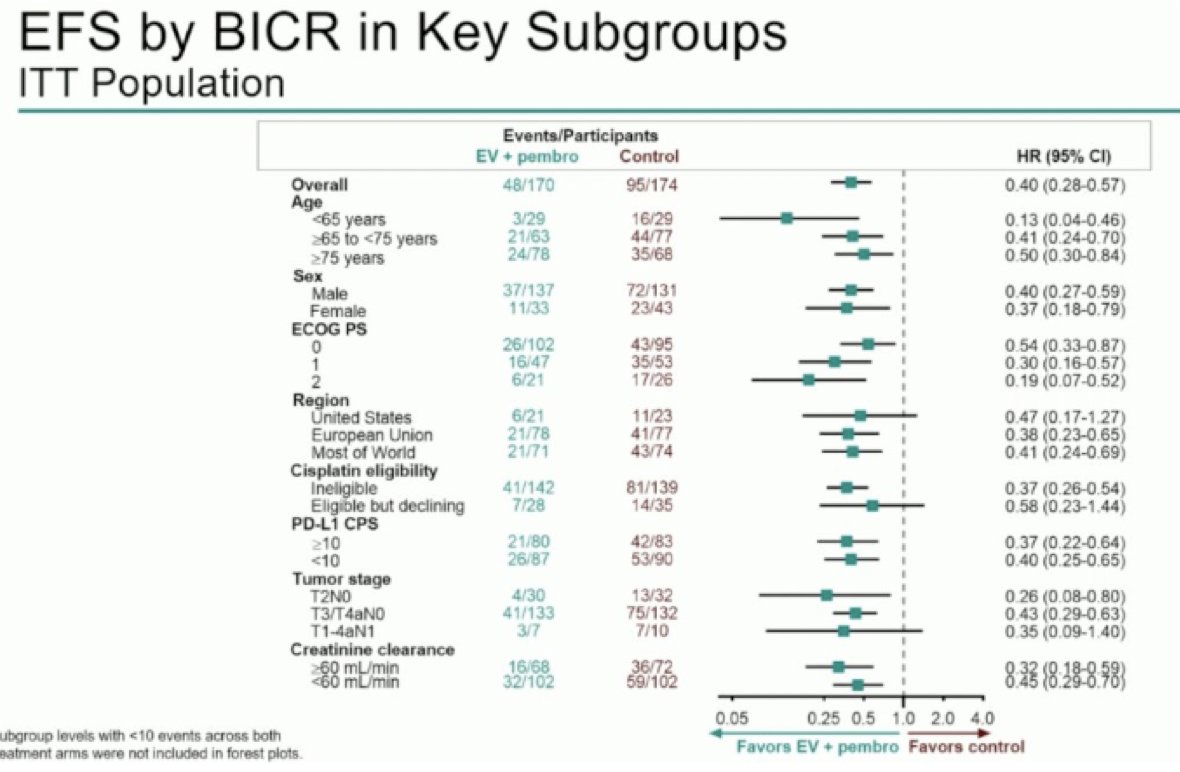
The event-free survival benefit with enfortumab vedotin + pembrolizumab was consistent across all predefined subgroups, including age, ECOG performance status, PD-L1 CPS, and tumor stage. The magnitude of benefit was maintained in both cisplatin-ineligible and cisplatin-declining patients, with hazard ratios favoring enfortumab vedotin + pembrolizumab across most subgroups:
The key secondary endpoint of overall survival reported a median of 41.7 months in the control arm versus not reached with enfortumab vedotin + pembrolizumab (HR 0.50, 95% CI 0.33–0.74; one-sided p = 0.0002), with early and sustained separation of the curves:

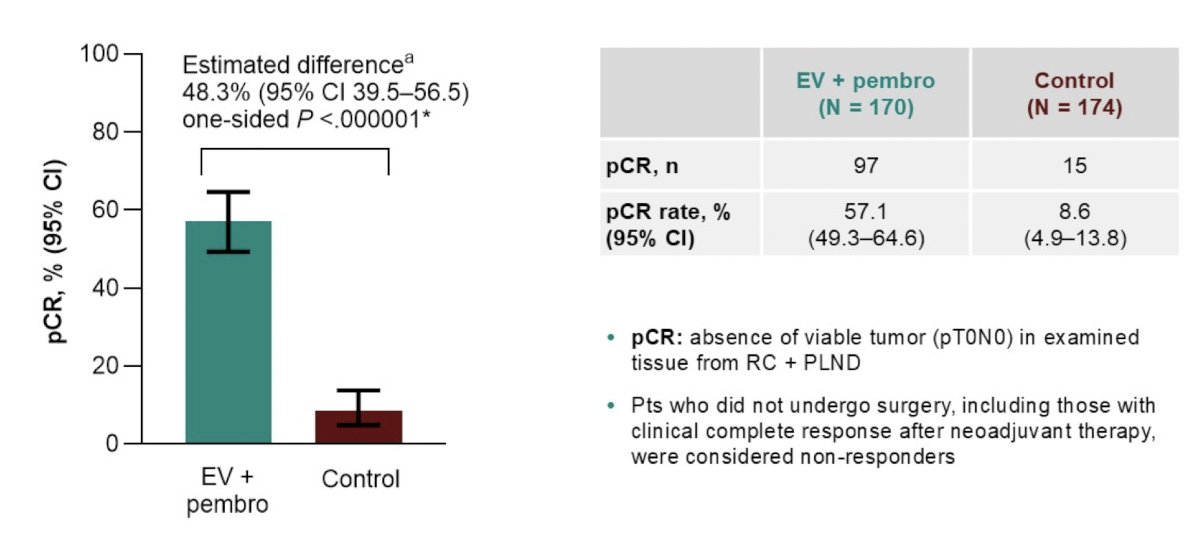
Pathological complete response, defined as the absence of viable tumor (pT0N0) in radical cystectomy specimens, was a key secondary endpoint of the study. The pathological complete response rate was 57.1% with enfortumab vedotin + pembrolizumab versus 8.6% with control (estimated difference 48.3%, one-sided p < 0.000001):
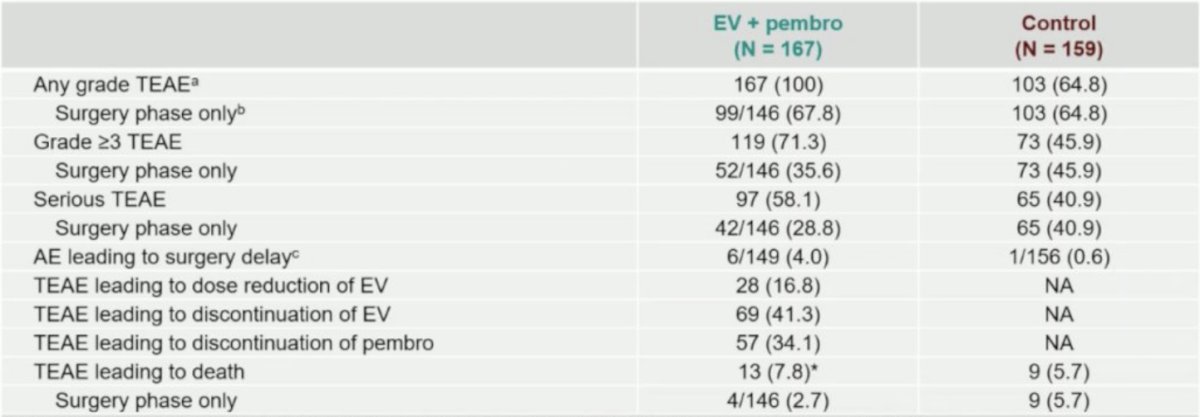
The median duration of neoadjuvant therapy with enfortumab vedotin + pembrolizumab was 1.6 months (range, 0.03–2.8) with a median of three cycles. The median adjuvant therapy duration was 8.0 months (range: 0.03–12.9), with six enfortumab vedotin and twelve pembrolizumab cycles. The safety profile was consistent with prior experience, with low rates of adverse events leading to surgical delay and no apparent increase in surgical complications, despite the frailty and comorbidities of this cisplatin-ineligible population:
Dr. Merrill notes that there are several limitations of KEYNOTE-905/EV-303, including that adjuvant immunotherapy was not routinely administered in the control arm, as nivolumab only became available midway through the trial (received by 16.7% of control patients), and depended on local access, reimbursement, and eligibility. Additionally, many patients in the control group likely did not have access to enfortumab vedotin + pembrolizumab upon relapse, which could have influenced overall outcomes. Adjuvant enfortumab vedotin + pembrolizumab was administered in 67% of patients who completed surgery, and most of those who started adjuvant therapy were able to complete it. These completion rates align with real-world practice, where a substantial proportion of patients do not proceed to adjuvant treatment due to postoperative recovery, comorbidities, or logistical barriers. Compared to NIAGARA,4 where 81% of surgical patients received adjuvant durvalumab, this highlights that while feasible, the adjuvant component of perioperative therapy may be more challenging to deliver outside of clinical trial settings. As data mature, understanding the degree of benefit derived from the neoadjuvant versus adjuvant phase will be key to optimizing future trial design.
To finish her presentation, Dr. Merrill discussed key components to successfully administering checkpoint inhibitors in clinical practice:
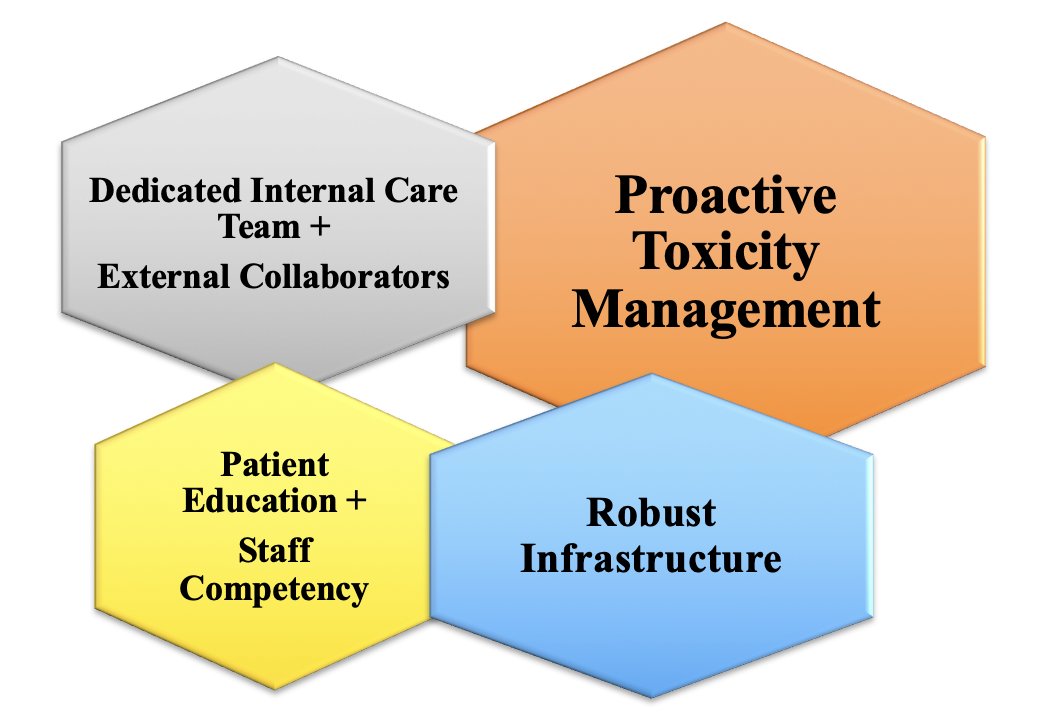
First, there is a dedicated internal care team plus external collaborators. Multidisciplinary care coordination is important, given the complexity of immune-related adverse events, which can affect any organ and necessitate a highly coordinated team that extends beyond the oncology clinic. The internal team includes oncologists, advanced practice providers, and oncology nurses who are experts in immunotherapy. Community infusion nurses, who see patients frequently, are critical for continuous monitoring and reporting of potential immune-related adverse events. For
external collaboration, it is important to establish relationships with specialists outside of oncology, as immune-related adverse events can mimic autoimmune diseases. This includes providers in emergency medicine, primary care, dermatology, gastroenterology, endocrinology, and rheumatology. The team should maintain an on-call roster of specialists experienced with immune-related adverse event management.
Second, there is proactive toxicity management. Due to the autoimmune nature of immune-related adverse events, prompt recognition and appropriate management are necessary to prevent severe and potentially fatal complications. Providers should have a high index of suspicion, in that all new or worsening symptoms should be considered treatment-related until proven otherwise. Clinical practice guidelines, such as those from ASCO,6 provide a graded approach to immune-related adverse event management based on the CTCAE:
- Grade 1 toxicities: Continue immune checkpoint inhibitors with close monitoring
- Grade 2 toxicities: Hold immune checkpoint inhibitors and consider resuming after the event resolves to Grade 1 or less. These patients may require corticosteroids
- Grade 3 toxicities: Hold immune checkpoint inhibitors and start high-dose corticosteroids. Further immunosuppression may be needed
- Grade 4 toxicities: Permanently discontinue immune checkpoint inhibitors (with rare exceptions, such as endocrine issues managed with hormone replacement)
For monitoring, patients should undergo regular blood work, including liver and thyroid function tests, which should be performed before each cycle.
Third, having a robust infrastructure. The community practice needs to be equipped to support immune checkpoint inhibitor therapy and its associated risks. Triage systems establish a triage line staffed by specialized oncology nurses who can help manage symptom calls after hours and on weekends. Standardized protocols provide clear, evidence-based protocols for administering immune checkpoint inhibitors, managing infusion reactions, and handling immune-related adverse events, which are essential for consistent, safe care. Additionally, data tracking allows standardized reporting of immune-related adverse events and tracking patient outcomes to help improve overall safety and treatment strategies.
Fourth, is patient education and staff competency. Given the rapid evolution of immunotherapy, ongoing education for all staff is crucial to provide the best care and stay current with guidelines. Oncology nurses, advanced practice providers, and oncologists must have a deep understanding of immune checkpoint inhibitor mechanisms, administration protocols, and immune-related adverse events management. Empowering patients and caregivers with knowledge is critical for the early detection and management of immune-related adverse events, which can occur months or even years after treatment. Educational content should cover the mechanism of action for immune checkpoint inhibitors and the key differences from traditional chemotherapy. Patients need to understand the potential for immune-related adverse events and the importance of reporting new symptoms promptly. Several tools include (i) wallet cards, which is an emergency contact card with the patient's immune checkpoint inhibitor information, potential side effects, and urgent contact numbers, which is essential for any healthcare provider, especially for emergency room visits, and (ii) written materials, such as handouts and online resources that are needed to reinforce verbal education. Importantly, initial education before treatment must be reinforced at every visit throughout the treatment and survivorship phases.
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter
References:
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naïve, high-risk non-muscle invasive bladder cancer: The randomized phase 3 CREST trial. Nat Med. 2025 Aug;31(8):2806-2814.
- De Santis M, Palou Redorta J, Nishiyama H, et al. Durvalumab in combination with BCG for BCG-naïve, high-risk, non-muscle-invasive bladder cancer (POTOMAC): Final analysis of a randomized, open-label, phase 3 trial. Lancet. 2025 Oct 17:S0140-6736(25)01897-5 [Epub ahead of print].
- Roupret M, Bertaut A, Pignot G, et al. ALBAN (GETUC-AFU 37): A phase 3, randomized, open-label, international trial of intravenous atezolizumab and intravesical Bacillus Calmette-Guerin (BCG) versus BCG alone in BCG-naïve high-risk, non-muscle invasive bladder cancer (NMIBC). Ann Oncol. 2025 Dec 31:S0923-7534(25):04787-8 [Epub ahead of print].
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(1):1773-1786.
- Pfister C, Gravis G, Flechon A, et al. Dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin or gemcitabine and cisplatin as perioperative chemotherapy for patients with nonmetastatic muscle-invasive bladder cancer: Results of the GETUG-AFU V05 VESPER trial. J Clin Oncol. 2022 Jun 20;40(18):2013-2022.
- Schneider BJ, Naidoo J, Santomasso BD, et al. Management of Immune-Related Adverse Events in Patients Treated with Immune Checkpoint Inhibitor Therapy: ASCO Guideline Update. J Clin Oncol. 2021 Dec 20;39(36):4073-4126.