Dr. Piyush Agarwal discussed current treatment options and future directions in non–muscle-invasive bladder cancer, noting that disease staging is based on depth of penetration, with NMIBC encompassing carcinoma in situ (CIS), Ta, and T1 disease.
Grade of disease is based on microscopic features and the architecture of cells, and is divided into low-grade and high-grade disease. Of note, 70% of bladder tumors are non-muscle invasive at the time of presentation. Risk grouping according to the EAU, AUA, and NICE is as follows: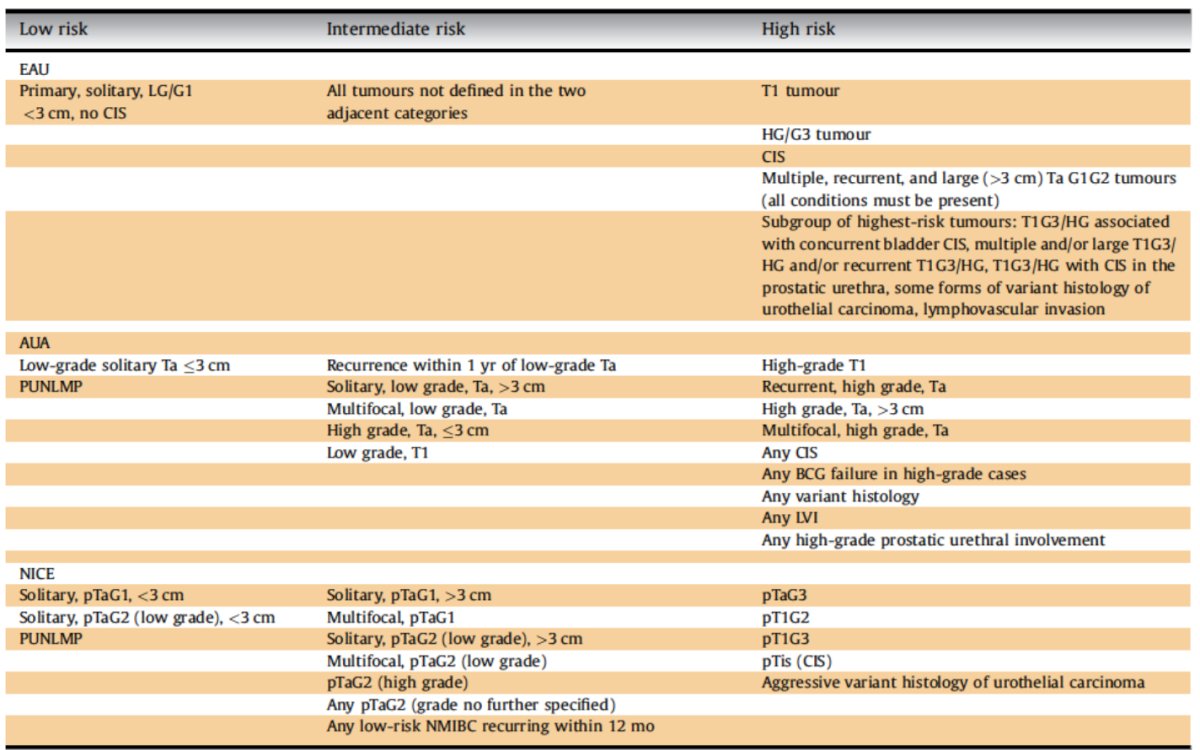
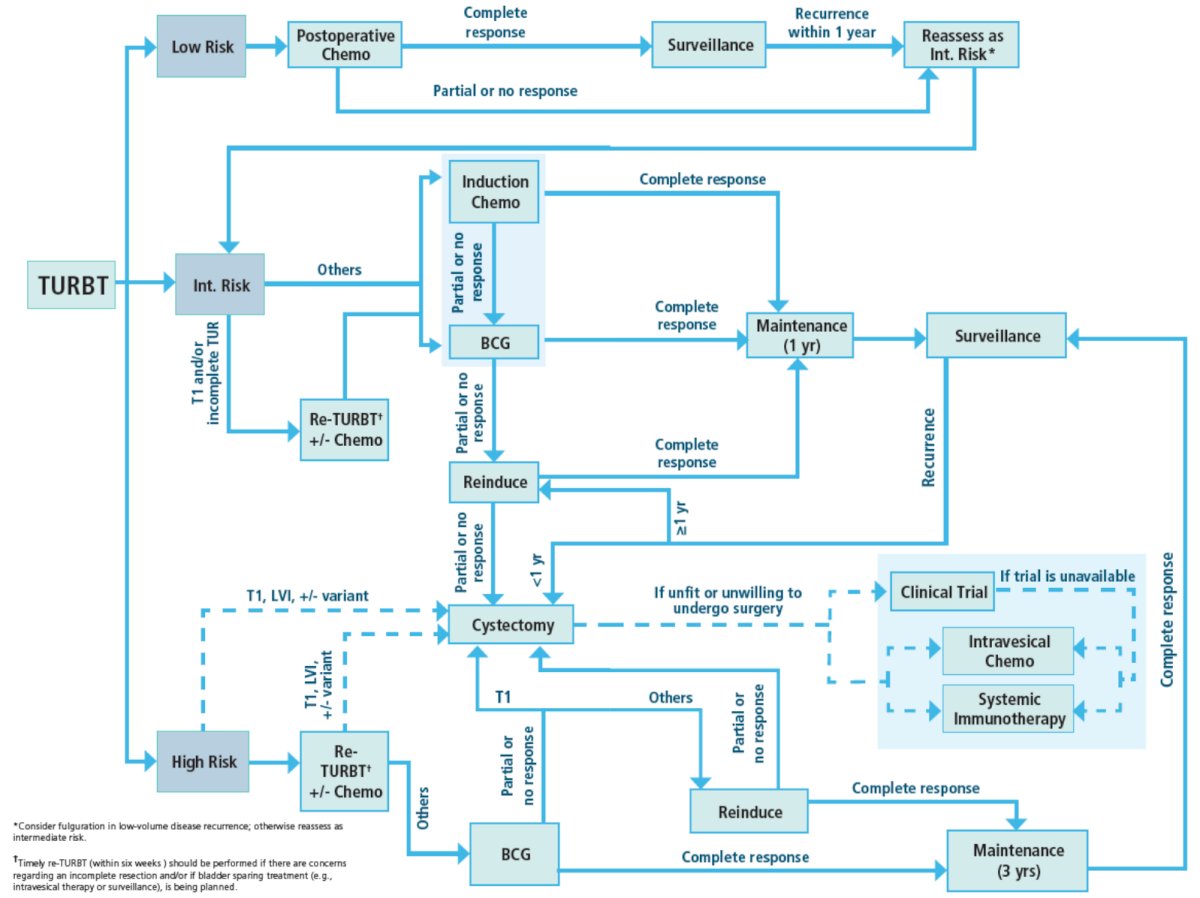
The AUA/SUO treatment algorithm includes the following for non-muscle invasive bladder cancer:
Dr. Agarwal then discussed intermediate risk non-muscle invasive bladder cancer, which is associated with a recurrence rate as high as 51% at 60 months, but with progression rates of only ~4%. However, recurrence risk decreases with longer interval of freedom of disease from TURBT.
In a multicenter assessment of gemcitabine + docetaxel in intermediate risk disease, Tan et al. evaluated oncological outcomes for 182 patients treated with BCG (n = 100) or intravesical sequential gemcitabine and docetaxel (n = 82).1 Notably, recurrence rates were similar in the two treatment groups (HR 1.06, 95% CI 0.65-1.73; p = 0.8): 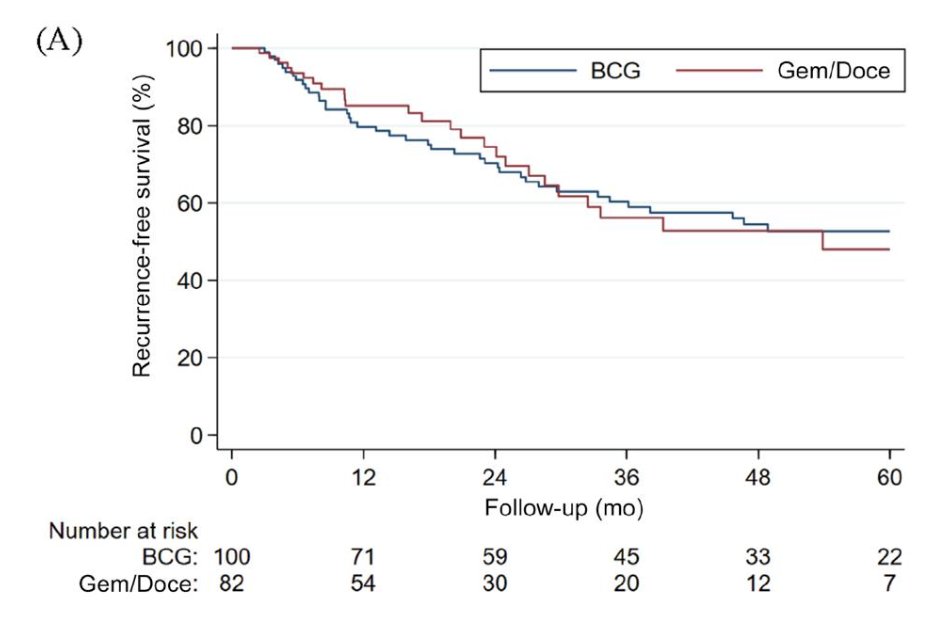
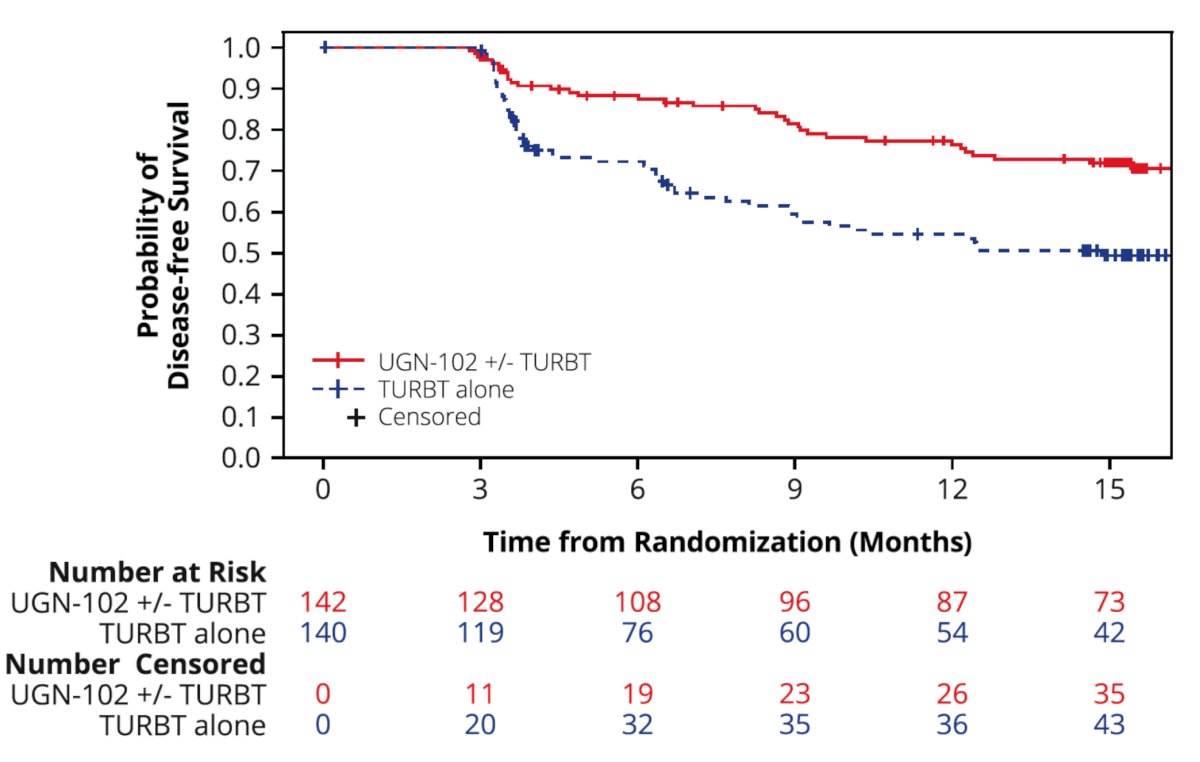
UGN-102 is a novel, reverse-thermal hydrogel formulation of mitomycin C designed for intravesical chemoablation of recurrent, low-grade intermediate risk non-muscle invasive bladder cancer. The ATLAS trial was a prospective, phase III, randomized, open-label trial that randomized patients with low-grade intermediate risk non-muscle invasive bladder cancer 1:1 to either UGN-102 +/- TURBT or TURBT alone (no adjuvant therapy).2 Patients in the UGN-102 arm who achieved a complete response at 3 months received no further treatment, whereas those with residual low-grade disease in either treatment arm underwent a TURBT for any remaining lesions. The primary study endpoint was disease-free survival. Among 282 patients, 142 and 140 were randomized to UGN-102 +/- TURBT and primary TURBT, respectively. Of the 142 patients randomized to UGN-102, 132 (96%) completed all six instillations. A 3-month complete response was observed in 65% (95% CI: 56–73%) of patients in the UGN-102 +/- TURBT arm, and 64% (95% CI: 55–72%) in the TURBT alone arm. Disease progression at the 3-month assessment was noted in 12 UGN-102 patients and 9 TURBT patients. Disease-free survival 15 months after randomization was estimated to be 72% for patients in the UGN-102 ± TURBT arm and 50% for patients in the TURBT monotherapy arm, with a hazard ratio of 0.45:
Dr. Agarwal emphasized the following criticisms of the ATLAS trial:
- Lack of adjuvant therapy in the control arm
- The standard of care arm did not receive adjuvant therapy (either single-dose perioperative chemotherapy or post-operative induction and maintenance intravesical chemotherapy)
- However, peri-operative chemotherapy (mitomycin or gemcitabine) is only given in up to 35–40% cases
- SWOG 0337 – similar 20% absolute risk reduction seen with single post-operative instillation of gemcitabine compared to saline
- However, SWOG had more low-risk, low-volume non-muscle invasive bladder cancer and likely fewer intermediate-risk patients
- The standard of care arm did not receive adjuvant therapy (either single-dose perioperative chemotherapy or post-operative induction and maintenance intravesical chemotherapy)
- Cost: extrapolation for a 6-week treatment using UGN-101 data = $140,000
- Indication: unclear from data if any size threshold for chemoablation to be effective
Dr. Agarwal then discussed the ENVISION trial,3 an ongoing, multinational, single-arm, phase III trial in patients with a biopsy-proven recurrence of untreated low-grade intermediate-risk non-muscle invasive bladder cancer. Eligible patients received 6 weekly intravesical instillations of UGN-102 and were evaluated at three months. Of 240 patients enrolled, the 3-month complete response rate was 79.2%, with an 82.3% (95% CI 74–86%) probability of a maintained response at 12 months:
![Dr. Agarwal then discussed the ENVISION trial [3], an ongoing, multinational, single-arm, phase III trial in patients with a biopsy-proven recurrence of untreated low-grade intermediate-risk non-muscle invasive bladder cancer. Eligible patients received 6 weekly intravesical instillations of UGN-102 and were evaluated at three months. Of 240 patients enrolled, the 3-month complete response rate was 79.2%, with an 82.3% (95% CI 74–86%) probability of a maintained response at 12 months:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-nmibc---navigating-the-options-and-future-directions/image-4.jpg)
FGFR alterations are present in ~50-80% of low-grade non-muscle invasive bladder cancer, and these alterations may function as oncogenic drivers. Erdafitinib is a selective pan-FGFR tyrosine kinase inhibitor. Oral erdafitinib is approved in the United States for the treatment of adults with locally advanced or metastatic urothelial carcinoma with susceptible FGFR3 alterations following progression on or after ≥1 prior systemic treatment. Oral erdafitinib has demonstrated anti-tumor activity in intermediate- and high-risk non-muscle invasive bladder cancer populations, limited by challenging systemic toxicities.4 TAR-210 is a novel intravesical erdafitinib-releasing system designed for sustained local delivery of therapy over 3 months in the bladder and is inserted using a urinary placement catheter in a brief in-office procedure:![FGFR alterations are present in ~50-80% of low-grade non-muscle invasive bladder cancer, and these alterations may function as oncogenic drivers. Erdafitinib is a selective pan-FGFR tyrosine kinase inhibitor. Oral erdafitinib is approved in the United States for the treatment of adults with locally advanced or metastatic urothelial carcinoma with susceptible FGFR3 alterations following progression on or after ≥1 prior systemic treatment. Oral erdafitinib has demonstrated anti-tumor activity in intermediate- and high-risk non-muscle invasive bladder cancer populations, limited by challenging systemic toxicities [4]. TAR-210 is a novel intravesical erdafitinib-releasing system designed for sustained local delivery of therapy over 3 months in the bladder and is inserted using a urinary placement catheter in a brief in-office procedure:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-nmibc---navigating-the-options-and-future-directions/image-5.jpg)
In a first-in-human study, TAR-210 was well-tolerated, with encouraging clinical activity in FGFR-altered intermediate-risk non-muscle invasive bladder cancer. The 12-week complete response rate was 90%, with a 9-month duration of response of 89%.
MoonRISe-1 is an open-label, multicenter, randomized phase III trial designed to evaluate the efficacy and safety of TAR-210 versus intravesical chemotherapy in patients with histologically confirmed, FGFR-altered, low-grade, intermediate-risk non-muscle invasive bladder cancer (n = 540). Evaluation of FGFR2/3 alteration status is performed using central or local tissue or urine testing. Eligible participants will undergo 1:1 randomization to TAR-210 every 12 weeks for one year versus investigator’s choice of intravesical chemotherapy (mitomycin or gemcitabine) every week for 4–6 doses (induction), followed by maintenance for 6 months to 1 year. The primary endpoint is disease-free survival, with secondary endpoints of:
- Time to next-line treatment
- High-grade recurrence-free survival
- Progression-free survival
- Rate of diagnostic and therapeutic urological interventions
- Safety and tolerability

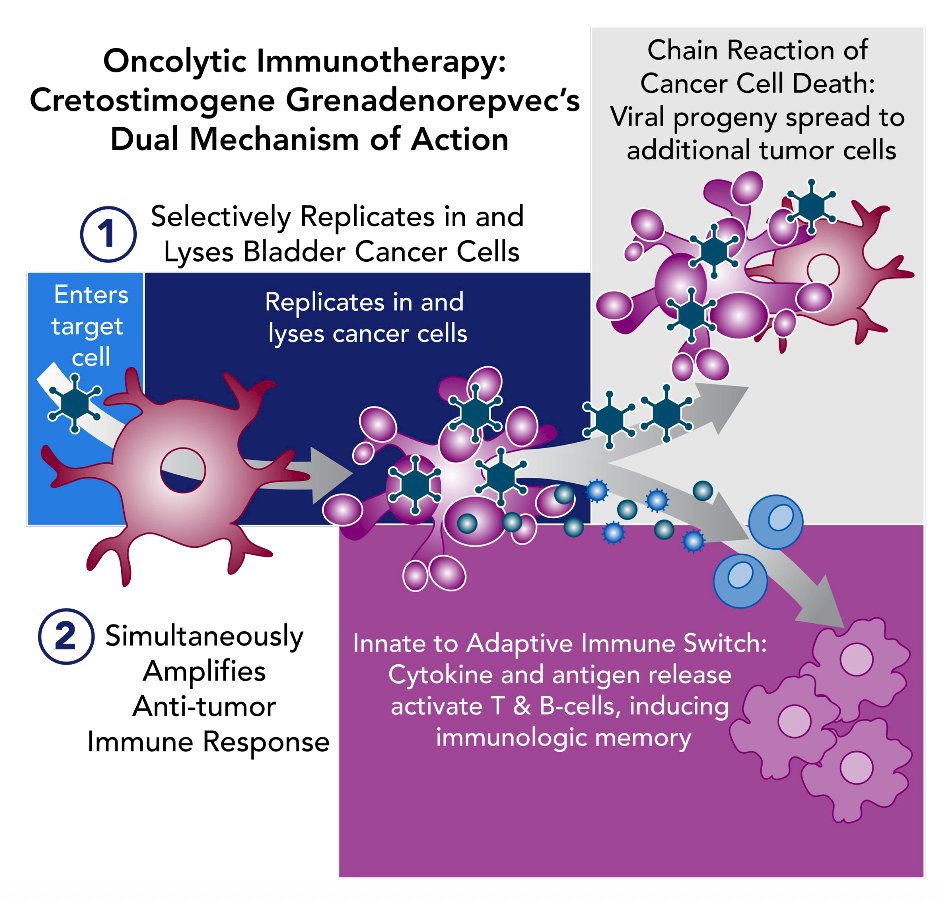
PIVOT-006 is an ongoing phase 3, randomized study of adjuvant intravesical cretostimogene grenadenorepvec versus surveillance for the treatment of intermediate risk non-muscle invasive bladder cancer. Cretostimogene grenadenorepvec, an oncolytic immunotherapy, selectively replicates in and lyses cancer cells with Rb-E2F pathway alterations, releasing antigens that initiate antitumor immune activation, further amplified by the GM-CSF transgene:
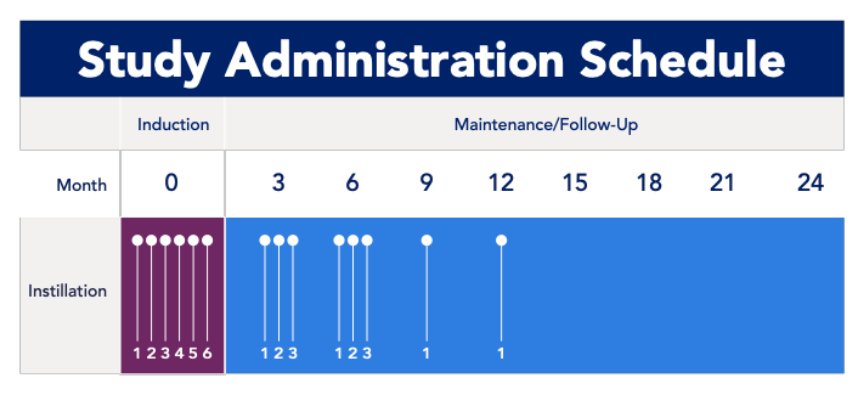
Eligibility criteria for PIVOT-006 include a histologically confirmed intermediate risk non-muscle invasive bladder cancer diagnosis within 90 days of randomization, as defined by AUA/SUO guidelines. Stratification factors include receipt of single-dose perioperative chemotherapy and tumor grade. Patients (n ~ 364) will be randomized 1:1 to undergo surveillance or to receive intravesical cretostimogene following TURBT. If intermediate risk non-muscle invasive bladder cancer recurrence is noted in the surveillance arm, patients will be eligible to receive intravesical cretostimogene. Intravesical cretostimogene is administered in combination with n-dodecyl-β-D-maltoside (DDM), an excipient that enhances adenoviral delivery, for 6 weekly doses during the induction phase, followed by 3 weekly maintenance cycles at months 3 and 6, and culminating in a single intravesical dose at months 9 and 12. Primary disease assessments include serial cystoscopy, urine cytology, axial imaging, and centralized review of pathologic samples:
The primary endpoint is recurrence-free survival, and secondary outcomes include safety, tolerability, progression-free survival, and time to next intervention. Exploratory outcome measures include health-related quality of life and biomarker analyses. 90+ clinical sites, including diverse representations across private practice and academic institutions, were selected for the trial. Enrollment for PIVOT-006 is complete.
Dr. Agarwal summarized intermediate risk non-muscle invasive bladder cancer with the following take-home messages:
- The recommendation is for TURBT with perioperative chemotherapy
- 3-month cystoscopy identifying early recurrence is a poor prognostic feature
- For future recurrences, Dr. Agarwal notes that we should consider IBCG Risk Stratification and discuss various strategies such as:
– Surveillance (0 risk factors)
– TURBT with perioperative chemotherapy (0 risk factors)
– UGN-102
– TURBT followed by:
• Induction and maintenance chemotherapy × 1 year
• Induction and maintenance BCG × 1 year
– Clinical trials
• FGFR3 alternation: TAR-210
• PIVOT-006: Cretostimogene
High Risk Non-Muscle Invasive Bladder Cancer (BCG-Naïve)
Dr. Agarwal discussed the history of BCG, which started with a 1929 autopsy study showing a lower frequency of cancer in patients with active or healed tuberculosis. This was followed in 1975 by Dr. de Kernion demonstrating treatment of isolated melanoma in the bladder of patients receiving intravesical BCG. Subsequently, in 1976, Dr. Morales reported the first successful use of intravesical BCG for the treatment of superficial urothelial carcinoma. This included using 6 doses at 120 mg/dose since this was the tolerated intradermal dose. Dr. Morales advocated for weekly instillation given that the adverse effects diminished in less than 1 week. In 1978, Dr. Morales treated 10 patients, noting that BCG reduced/eradicated tumor recurrences in 7 patients. This was followed by 2 randomized controlled trials, including the SWOG and MSKCC trials, which confirmed reduced tumor recurrence compared to TURBT alone. Subsequently, in 1990, the FDA approved intravesical BCG.
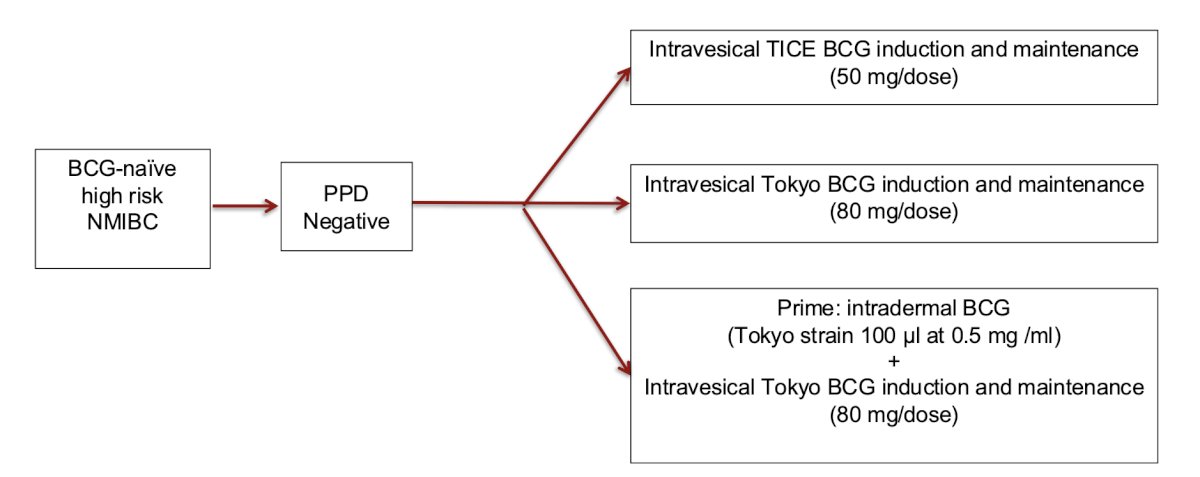
Secondary to the BCG shortage, there has been increased interest in using new strains of BCG. The PRIME (S1602) trial is a randomized phase III study designed to evaluate the effectiveness of different BCG regimens in patients with CIS, high-grade Ta, or high-grade T1 non-muscle invasive bladder cancer. A total of 969 patients will be randomized across three arms:
- Intravesical BCG TICE strain (50 mg/dose)
- Intravesical BCG Tokyo strain (80 mg/dose)
- Priming arm: Intradermal Tokyo BCG (100 µL at 0.5 mg/mL) administered prior to intravesical BCG Tokyo strain (80 mg/dose)
Several studies have assessed the impact of the BCG shortage. A retrospective study from France compared two cohorts of patients: from 2013-2016 during the BCG shortage versus from 2011-2013 during the pre-BCG shortage.5 During the BCG shortage, all high-risk patients were treated with induction BCG only (no maintenance), and all intermediate-risk risk with mitomycin C. The 24-month recurrence rate was 46.9% versus 16.2% (pre-BCG shortage; p < 0.001), and the cystectomy rate was 7.1% versus 1.5% (p = 0.005). This study found that the increased cost of management was estimated at 783 Euros per patient with a new diagnosis of non-muscle invasive bladder cancer.
The NIMBUS trial6 assessed whether a reduced number of standard-dose BCG instillations is noninferior to the standard number and dose in patients with high-grade non-muscle invasive bladder cancer. There were 345 patients randomized to the standard BCG schedule [6 weeks of induction followed by 3 weeks of maintenance at 3, 6, and 12 months (15 instillations)] versus the reduced frequency BCG schedule [induction at weeks 1, 2, and 6 followed by 2 weeks (weeks 1 and 3) of maintenance at 3, 6, and 12 months (9 instillations)]. After 12 months of median follow-up, the intention-to-treat analysis showed a safety-relevant difference in recurrences between treatment arms: 46/170 (reduced frequency) versus 21/175 patients (standard). Additional safety analyses showed a hazard ratio of 0.40 with the upper part of the one-sided 97.5% confidence interval of 0.68, meeting a predefined stopping criterion for inferiority.
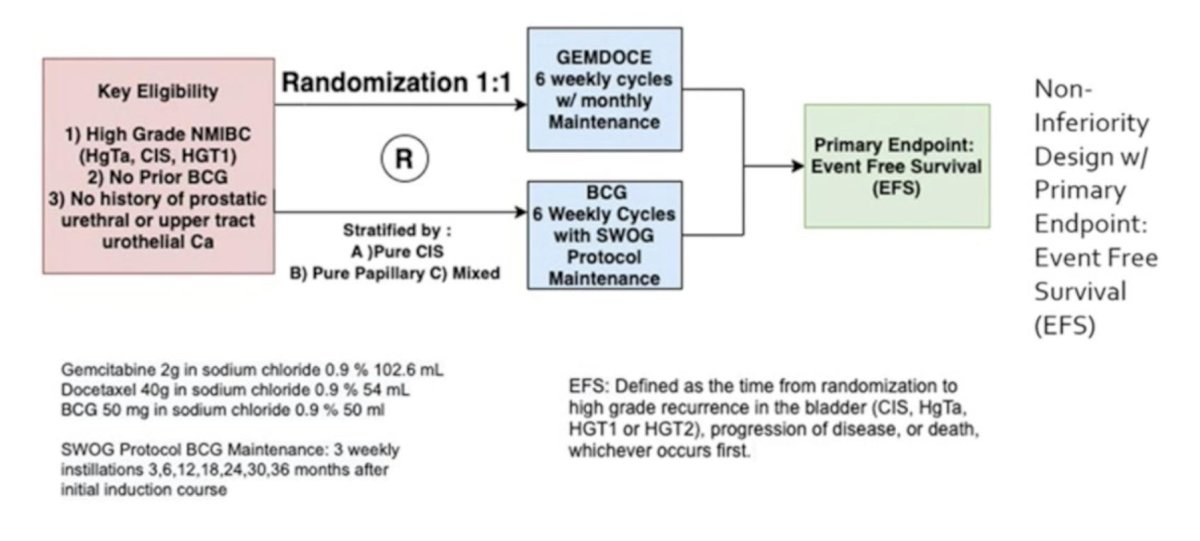
There are several strategies for the BCG shortage proposed by Dr. Agarwal. First, perhaps we can complete 4 weeks of BCG for induction instead of 6, based on the BCAN/COVID-19 expert opinion. However, the caveat is that 6 weeks are still important in those not previously immunized against mycobacterial antigens. Second, perhaps we can reserve maintenance BCG for high-risk patients (CIS, T1) and dose at 1/3 dose in order to be able to treat 3 patients concurrently. Third, perhaps we can reserve BCG for high-risk patients, and treat intermediate-risk patients with intravesical chemotherapy in the first-line setting, which is supported by the AUA/SUO, EAU, and NCCN guidelines. Fourth, perhaps we can use primary intravesical chemotherapy for all patients. Dr. Agarwal notes that at the University of Chicago, during the BCG shortage, among BCG naïve patients treated with gemcitabine + docetaxel (16 HG Ta, 12 HG T1, 5 CIS), the 2-year recurrence-free survival rate was 88% for HG Ta, 80% for HG T1, and 80% for CIS. Ultimately, we await the results of the BRIDGE trial assessing BCG versus gemcitabine + docetaxel in high-risk BCG naïve non-muscle invasive bladder cancer:
The CREST trial7 was presented at AUA 2025, which was a three-arm study comparing different combinations of sasanlimab and BCG. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause:
![The CREST trial [7] was presented at AUA 2025, which was a three-arm study comparing different combinations of sasanlimab and BCG. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-nmibc---navigating-the-options-and-future-directions/image-11.jpg)
The risk of experiencing an event-free survival event was 32% lower with sasanlimab + BCG compared to BCG induction and maintenance alone (stratified HR 0.68, 95% CI 0.49–0.94; 1-sided p-value: 0.0095). In patients with CIS, the probability of maintaining a complete response at 36 months was 91.7% with sasanlimab + BCG induction and maintenance, compared to 67.7% with BCG induction and maintenance alone:

High Risk Non-Muscle Invasive Bladder Cancer (BCG Unresponsive)
The definitions of BCG failure are based on “adequate” BCG, which consists of: one induction course (at least 5 of 6 doses) + one maintenance course (at least 2 of 3 doses) or a second induction course (at least 2 of 6 doses). The BCG-failure population is defined as the following:
- BCG refractory: persistent high-grade non-muscle invasive bladder cancer at 6 months after adequate BCG
- BCG relapsing: recurrence of high-grade non-muscle invasive bladder cancer after achieving a disease-free state of 6 months after adequate BCG
- BCG unresponsive: BCG-refractory and BCG-relapsing within 12 months of prior exposure to BCG for CIS and 6 months of prior exposure to BCG for papillary tumors
In 2015, Steinberg et al.8 reported on an initial 45 patients with recurrent non muscle invasive bladder cancer after BCG treated with gemcitabine first, followed by docetaxel. These patients were treated with 6 weekly instillations and then monthly maintenance therapy for 2 years. Response rates were 66% at first surveillance, 54% at 1 year, and 34% at 2 years after induction therapy:
![In 2015, Steinberg et al. [8] reported on an initial 45 patients with recurrent non muscle invasive bladder cancer after BCG treated with gemcitabine first, followed by docetaxel. These patients were treated with 6 weekly instillations and then monthly maintenance therapy for 2 years. Response rates were 66% at first surveillance, 54% at 1 year, and 34% at 2 years after induction therapy:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-nmibc---navigating-the-options-and-future-directions/image-13.jpg)
The approval for pembrolizumab in BCG-unresponsive disease was based on the KEYNOTE-057 trial [9]. Patients received intravenous pembrolizumab 200 mg every 3 weeks for up to 24 months or until patients had evidence of centrally-confirmed disease persistence, recurrence, or progression or unacceptable drug-related toxicity:
![The approval for pembrolizumab in BCG unresponsive disease was based on the KEYNOTE-057 trial [9]. Patients received intravenous pembrolizumab 200 mg every 3 weeks for up to 24 months or until patients had evidence of centrally-confirmed disease persistence, recurrence, or progression or unacceptable drug-related toxicity:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-nmibc---navigating-the-options-and-future-directions/image-14.jpg)
Overall, among 101 patients, 64% of patients had CIS-only disease, and complete response was 46%, with a median duration of response of 16.2 (95% 6.7-36.2) months:
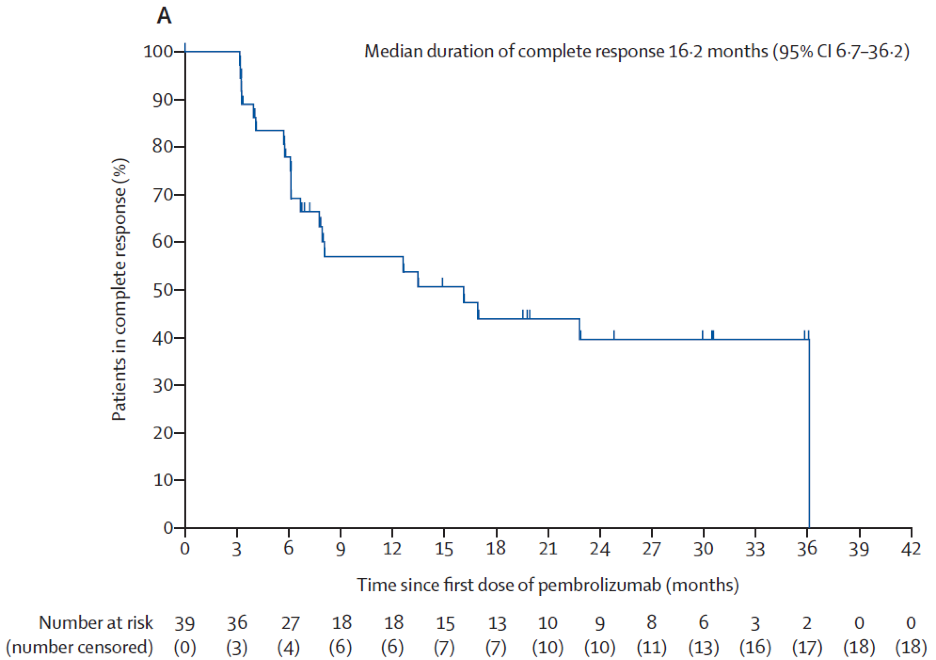
Moreover, 46% of complete responses were maintained at 12 months; unfortunately, only ~20% of all patients experienced a response of 12 months or greater.
Next, Dr. Agarwal discussed nadofaragene firadenovec, which was assessed in a phase 3, multicenter, open-label, repeat-dose study across 33 centers in the United States of 151 patients with BCG-unresponsive non-muscle invasive bladder cancer.10 This study met its primary endpoint with 53.4% of patients with CIS +/- papillary disease achieving a complete response at three months, with 24.2% maintaining this response by 12 months. This treatment was very tolerable, with only 2% discontinuing therapy due to adverse events. Additionally, patients were dosed with a single intravesical instillation every 3 months, but patients were not allowed re-induction. Nadofaragene firadenovec was approved by the FDA in 2022.
The Quilt 3032 trial11 led to the approval of N-803 (nogapendekin alfa inbakicept: ANKTIVA®), which is an interleukin-15 superagonist (IL-15) that promotes activation and proliferation of natural killer cells, CD8+ T cells, and memory T cells without expanding immunosuppressive T-reg cells. In this trial, over a median follow-up of 23.9 months, the complete response rate was 71% and the median duration of response was 26.6 months:
![The Quilt 3032 trial [11] led to the approval of N-803 (nogapendekin alfa inbakicept: ANKTIVA®), which is an interleukin-15 superagonist (IL-15), that promotes activation and proliferation of natural killer cells, CD8+ T cells and memory T cells without expanding immunosuppressive T-reg cells. In this trial, over a median follow up of 23.9 months, the complete response rate was 71% and the median duration of response was 26.6 months:](/images/com-doc-importer/240-lugpa-2025/lugpa-2025-nmibc---navigating-the-options-and-future-directions/image-16.jpg)
Based on these results, the FDA granted breakthrough approval of N-803 in April 2024.
The SunRISe-1 trial was published in July 2025 in Journal of Clinical Oncology5 and subsequently led to FDA approval of TAR-200 monotherapy on September 9, 2025, for BCG-unresponsive CIS with or without papillary disease. In the SunRISe-1 trial (cohort 2: TAR-200 monotherapy, CIS only), the complete response rate and median duration of response were 82.4% (95% CI, 72.6 to 89.8) and 25.8 months (95% CI, 8.3 to not estimable), respectively. Rates of grade ≥3 treatment-related adverse events were 12.9%, and of serious treatment-related adverse events were 5.9%:
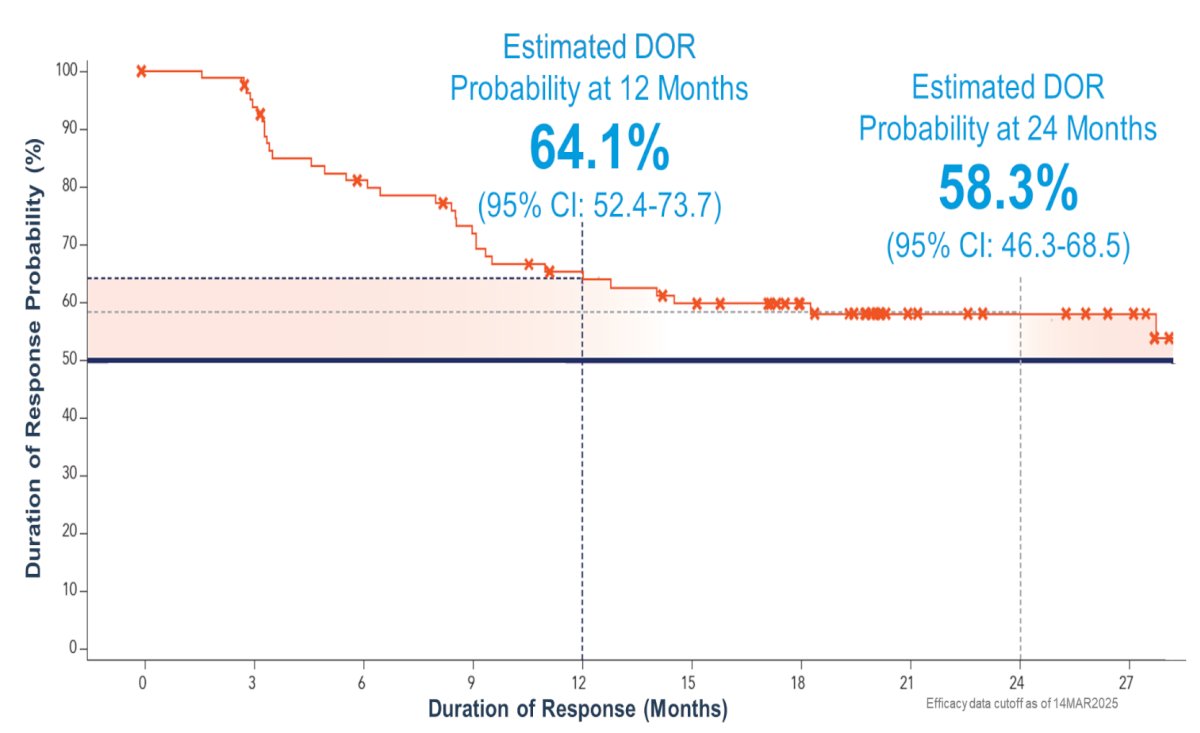
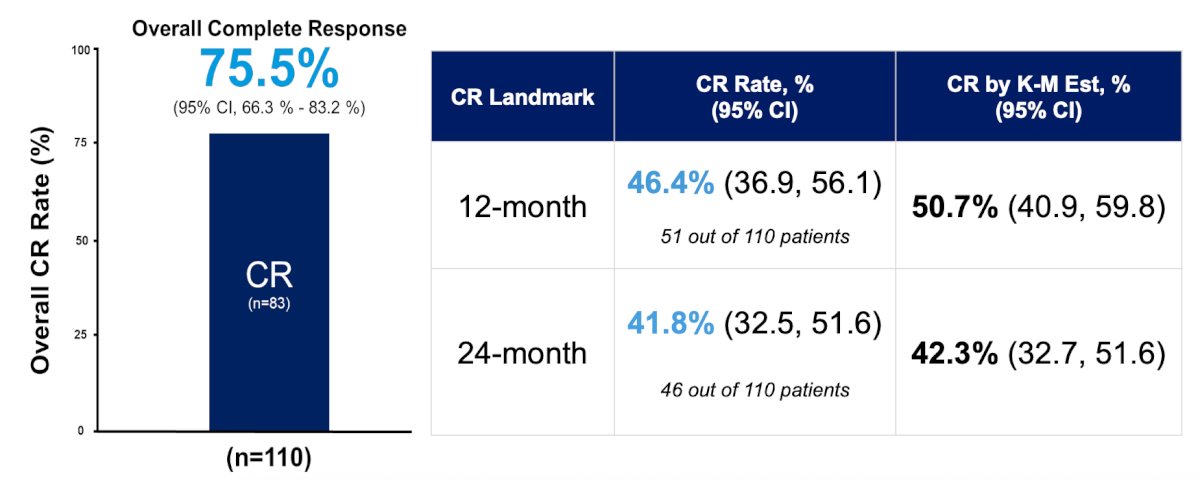
At the Western Section of the AUA annual meeting, Dr. Tyson reported final results from BOND-003 Cohort C, a phase 3, single-arm study of intravesical cretostimogene for high-risk BCG unresponsive non-muscle invasive bladder cancer with CIS. Overall, 112 adults with confirmed high-risk BCG-unresponsive non-muscle invasive bladder cancer with CIS were enrolled, with efficacy data from 110 patients. With a median follow-up time of 22.3 months, the complete response rate at any time is 75.5% (83/110) (95% CI 66.3-83.2%). Kaplan-Meier estimates of 12- and 24-month duration of response are 64.1% (95% CI 52.4-73.7%) and 58.3% (95% CI 46.3-68.5%), respectively, with an ongoing median duration of response of 27.9 months (95% CI 13.8% to not reached):
The 12-month complete response rate is 46.4% (51/110) (95% CI 36.9-56.1%). Landmark and Kaplan-Meier estimated 24-month complete response rates are 41.8% (46/110) (95% CI 32.5-51.6%) and 42.3% (95% CI 32.7-51.6), respectively. Complete responses are consistent across all patient subgroups:
At 24 months, 97.3% (107/110) are free from ≥T2 progression during the treatment phase, and 84.5% (93/110) have avoided radical cystectomy. There were 82.4% (14/17) of patients who underwent radical cystectomy and were T0 or non-muscle invasive bladder cancer on final pathology. Cretostimogene has a very well-tolerated safety profile, with no grade ≥3 treatment-related adverse events. Grade 1 and 2 related adverse events (ie, bladder spasm, pollakiuria, urgency) are transient, with a median resolution time of 1 day.
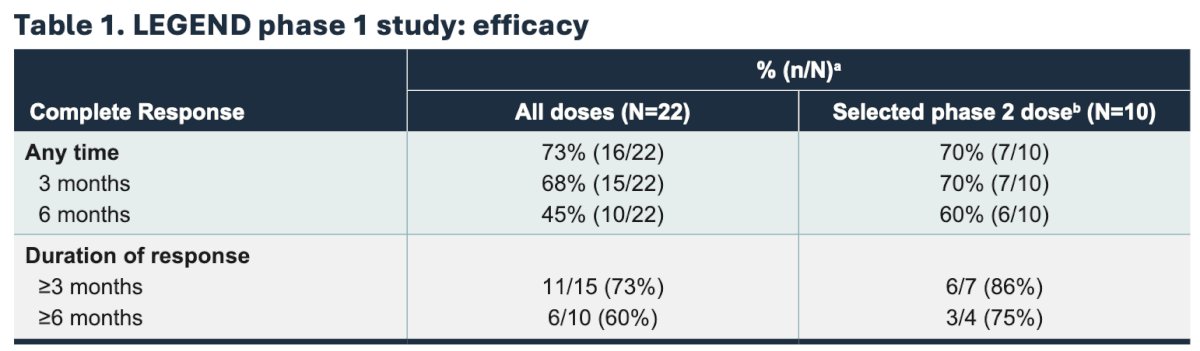
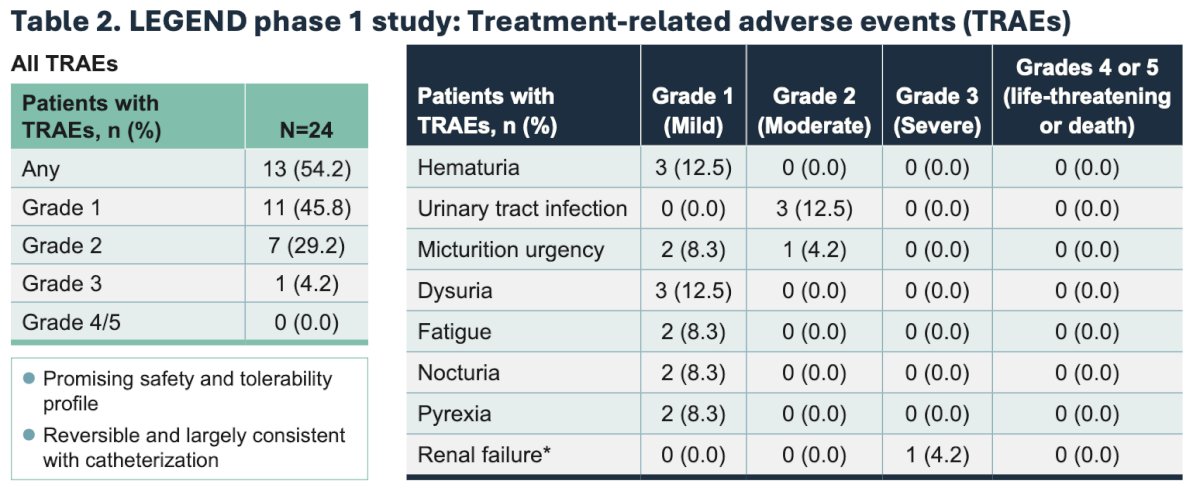
LEGEND is an ongoing, multicohort phase 1/2 study of detalimogene voraplasmid in patients with high-risk non-muscle invasive bladder cancer. Phase 1 patients include BCG-unresponsive non-muscle invasive bladder cancer with CIS with detalimogene voraplasmid dosing 2 or 4 doses over a 12-week cycle. The cohorts are a 3+3 dose escalation, with 3 dose levels (0.25 ng/mL, 0.8 mg/mL, 2.5 mg/mL) and two schedules (2 doses/12-week cycle versus 4 doses/12-week cycle). The primary endpoint is safety, and the secondary endpoint is efficacy at 3 months. Enrollment for phase 1 is now complete, and treatment with detalimogene voraplasmid resulted in a 73% complete response rate at any time, and a promising safety and tolerability profile. The safety and efficacy findings from the phase of LEGEND are summarized as follows:
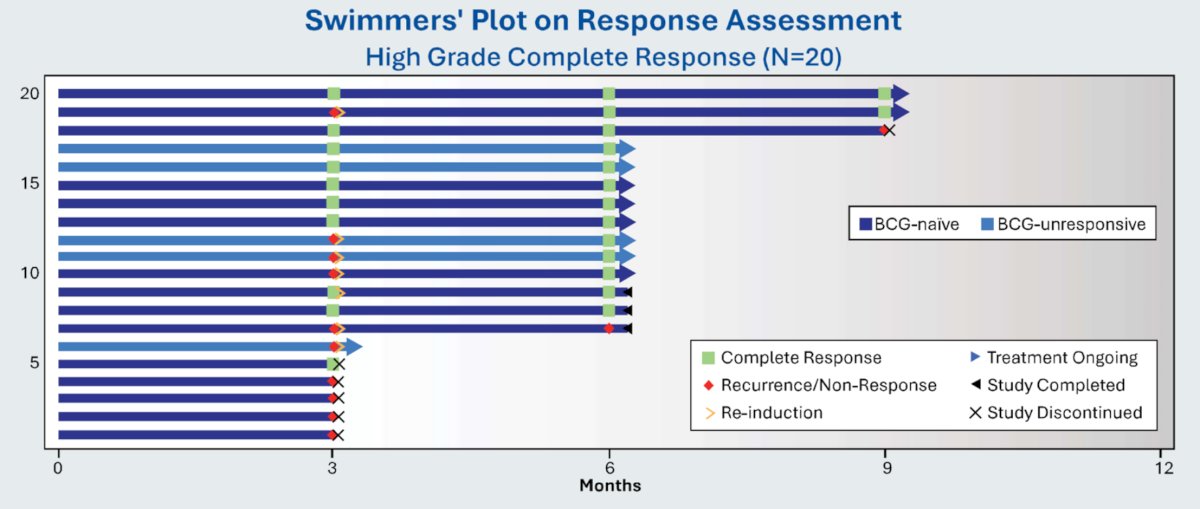
The ADVANCED-2 trial was initially presented at SUO 2024, utilizing TARA-002, a promising broad-spectrum immune potentiator that induces a TH1 pro-inflammatory cytokine response. TARA-002 is a lyophilized biological preparation for instillation containing cells of Streptococcus pyogenes (Group A, type 3) strain treated with benzylpenicillin. To date, 24 patients have been enrolled in the ADVANCED-2 study. Most patients had a baseline diagnosis of CIS only (58%), while 25% had CIS + Ta disease, and 17% had CIS + T1 disease.
For the primary objective, the rate of high-grade complete response at any time was 70% overall, with 80% for BCG-unresponsive subjects and 67% for BCG-naive subjects. At month 6, the rates of high-grade complete response were 72% overall, 100% for BCG-unresponsive subjects, and 64% for BCG-naive subjects:

The secondary objective was to assess the duration of response to TARA-002. A total of 9 subjects who were complete responders at month 3 and continued the study maintained response through month 6, as noted in the swimmer’s plot below. Notably, of the 5 subjects who did not achieve an initial complete response and received re-induction, the complete response rate at month 6 was 80%:
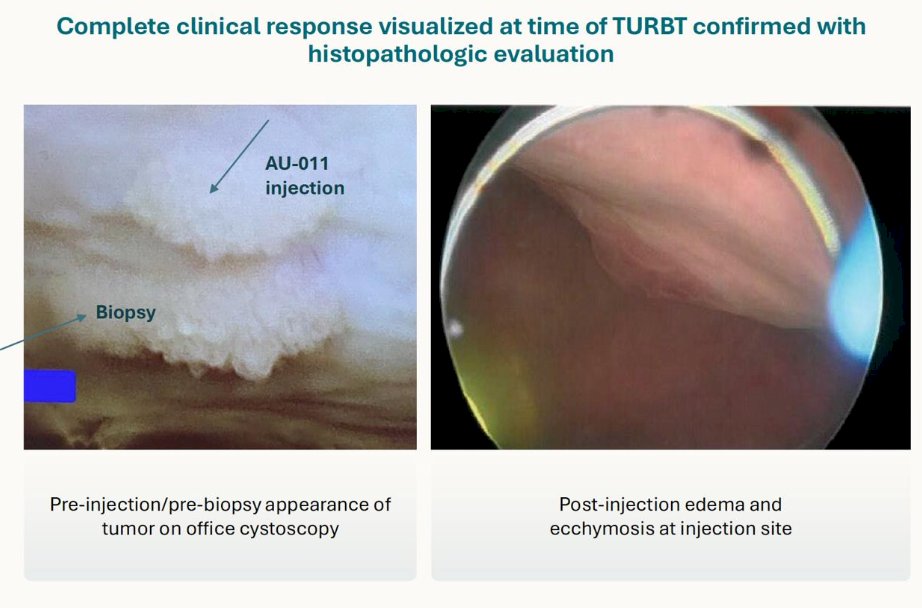
Finally, Dr. Agarwal discussed AU-011, which uses viral-like particles conjugated to a photosensitizer and is activated by near-infrared light. Cells are disrupted by reactive oxygen species and immune-mediated death. This is an ongoing phase 1 trial, with the following treatment/assessment schedule:
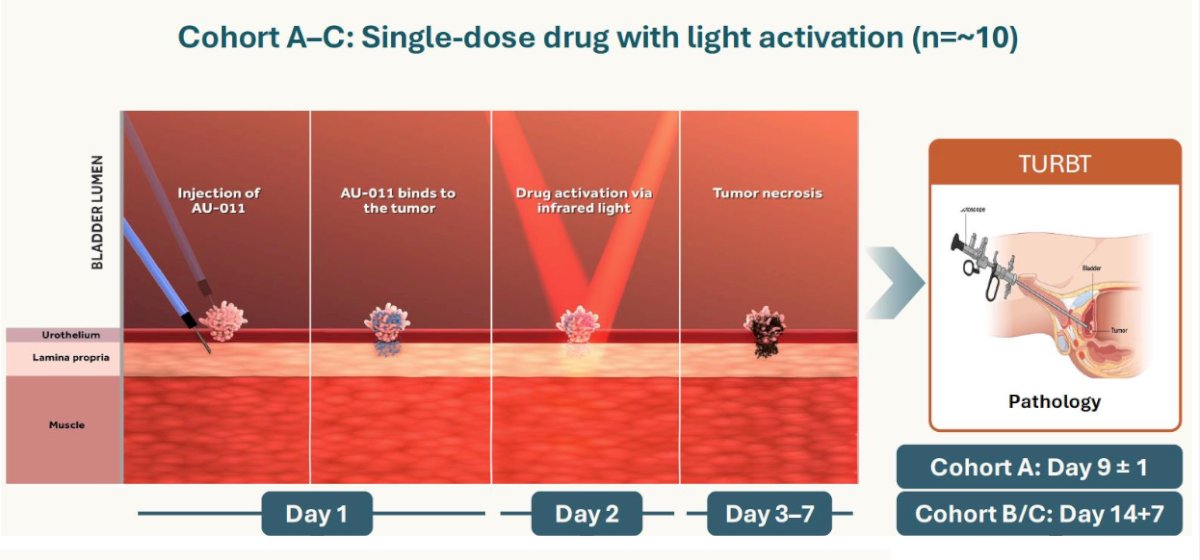
The initial results show impressive tumor regression and immunology:
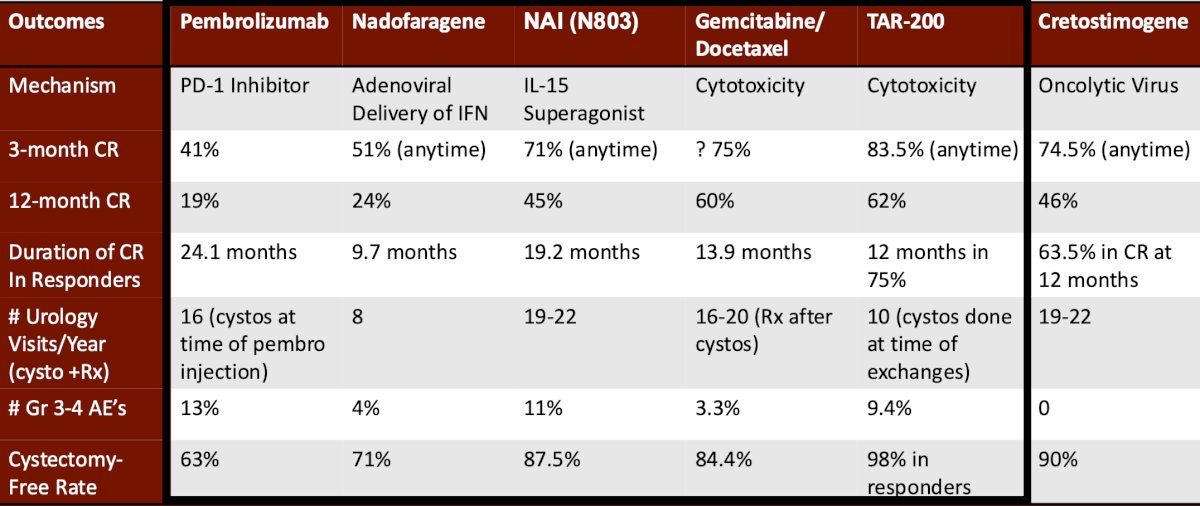
Dr. Agarwal summarized the BCG unresponsive disease space with the following summary table of trials and data that he collated:
Dr. Agarwal concluded his presentation discussing navigating the options and future directions of non-muscle invasive bladder cancer with the following take-home points:
- Risk stratification is important after TURBT to determine treatment
- Intermediate risk disease has active clinical trials and one new approved agent, along with effective standard of care options
- The high-risk BCG naïve disease space has new data showing improved event-free survival with the addition of subcutaneous PD-1 inhibitor, and data pending for the addition of a priming vaccine, other BCG strains, and comparison with gemcitabine/docetaxel
- High-risk BCG unresponsive – the standard of care is still radical cystectomy
- Historically, complete response rates with a third induction course of BCG after two failed prior induction courses is approximately 20–30% at 12 months [13]
- Gemcitabine/Docetaxel is widely adopted, effective, and relatively inexpensive
- Several novel agents have been approved:
- Complete response rates are high initially, but at 12 months, range from 20%–60%
- N803 and cretostimogene allowed for re-induction and salvaged ~50% of patients
- “Real-world practices” and biomarkers (ie, the Vesta test by Valar Labs) may drive the sequencing of agents
References:
- Tan WS, McElree IM, Davaro F, et al. Sequential intravesical gemcitabine and docetaxel is an alternative to Bacillus Calmette-Guerin for the treatment of intermediate-risk non-muscle invasive bladder cancer. Eur Urol Oncol. 2023 Oct;6(5):531-534.
- Prasad SM, Huang WC, Shore ND, et al. Treatment of low-grade intermediate-risk nonmuscle-invasive bladder cancer with UGN-102 +/- transurethral resection of bladder tumor compared to transurethral resection of bladder tumor monotherapy: A randomized, controlled, phase 3 trial (ATLAS). J Urol. 2023 Oct;210(4):619-629.
- Prasad SM, Shishkov D, Vladimirov Mihaylov N, et al. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer with UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025 Feb;213(2):205-216.
- Catto JWF, et al. Treatment patterns and outcomes in patients with FGFR-altered metastatic urothelial carcinoma: a multicenter observational study. Ann Oncol. 2024;35:98–106.
- Ourfali S, Ohannessian R, Fassi-Fehri H, et al. Recurrence rate and cost consequence of the shortage of Bacillus Calmette-Guerin Connaught Strain for Bladder Cancer Patients. Eur Urol Focus. 2021 Jan;7(1):111-116.
- Grimm MO, van der Heijden AG, Colombel M, et al. Treatment of high-grade non-muscle-invasive bladder carcinoma by standard number and dose of BCG instillations versus reduced number and standard dose of BCG instillations: Results of the European Association of Urology Research Foundation Randomized Phase III Clinical Trial “NIMBUS”. Eur Urol 2020 May 20:S0302-2838(20)30334-1.
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naïve, high-risk non-muscle invasive bladder cancer: The randomized phase 3 CREST trial. Nat Med. 2025 Aug;31(8):2806-2814.
- Steinberg RL, Thomas LJ, O’Donnell MA, et al. Sequential Intravesical Gemcitabine and Docetaxel for the Salvage Treatment of Non-Muscle Invasive Bladder Cancer. Bladder Cancer. 2015 Apr 30;1(1):65-72.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1).
- Daneshmand S, Van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guerin-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer: Results from the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025 Jul 30 [Epub ahead of print].
- Catalona WJ, Hudson MA, Gillen DP, et al. Risks and benefits of repeated courses of intravesical bacillus Calmette-Guerin therapy for superficial bladder cancer. J Urol. 1987 Feb;137(2):220-224.