(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the Plenary Session: Paradigm-Shifting, Practice-Changing Clinical Trials in Urology. Dr. Neal Shore discussed how Sasanlimab in combination with Bacillus Calmette-Guerin improves event-free survival versus Bacillus Calmette-Guerin as standard of care in high-risk non-muscle-invasive bladder cancer.
Dr. Shore began his presentation by highlighting that the standard of care for high-risk non-muscle invasive bladder cancer (HR-NMIBC) remains transurethral resection of bladder tumor (TURBT) followed by induction and maintenance Bacillus Calmette-Guérin (BCG) therapy. Despite this approach, approximately 40% of patients experience disease recurrence or progression within 24 months, facing an unfavorable prognosis. Treatment options offering durable disease control remain limited, particularly for patients with carcinoma in situ (CIS). Dr. Shore emphasized that combining a PD-1 inhibitor with BCG is supported by evidence of increased PD-L1 expression following BCG treatment. He introduced sasanlimab, a PD-1 inhibitor that has demonstrated durable anti-tumor activity and a manageable safety profile in patients with advanced or metastatic solid tumors.
At the Paradigm-Shifting, Practice-Changing Clinical Trials in Urology session, Dr. Shore presented the primary analysis of the phase 3 CREST study, which evaluated the superiority of subcutaneous sasanlimab in combination with BCG versus BCG monotherapy in patients with HR-NMIBC. Notably, the study was conducted entirely during the COVID-19 pandemic.
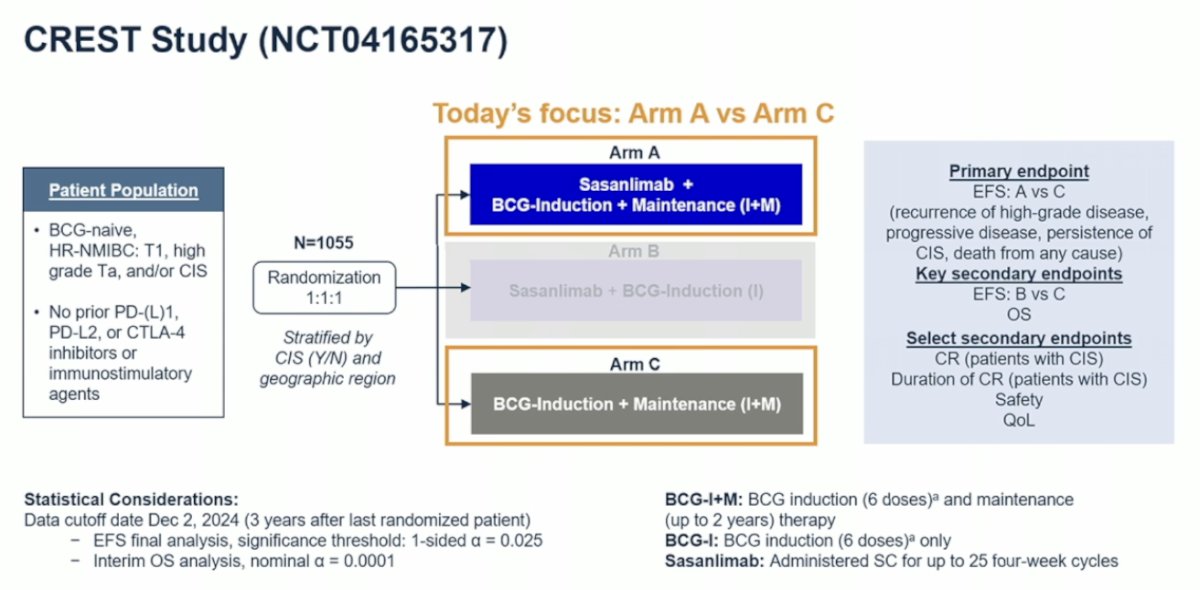
The study schema for CREST is outlined below. It is a three-arm study comparing different combinations of sasanlimab and BCG. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. For the presentation, the focus was on the comparison between Arm A and Arm C. The primary endpoint was event-free survival (EFS), defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause. Key secondary endpoints included EFS for Arm B versus Arm C and overall survival (OS). Additional select secondary endpoints included complete response (CR) in patients with CIS, duration of CR, safety, and quality of life (QoL).
Baseline characteristics were balanced and representative of the HR-NMIBC population. Notably, more than 55% of patients had T1 disease. Carcinoma in situ (CIS) was identified in over 14% of patients, and in more than 25% of cases, CIS was found concomitantly with papillary tumors.

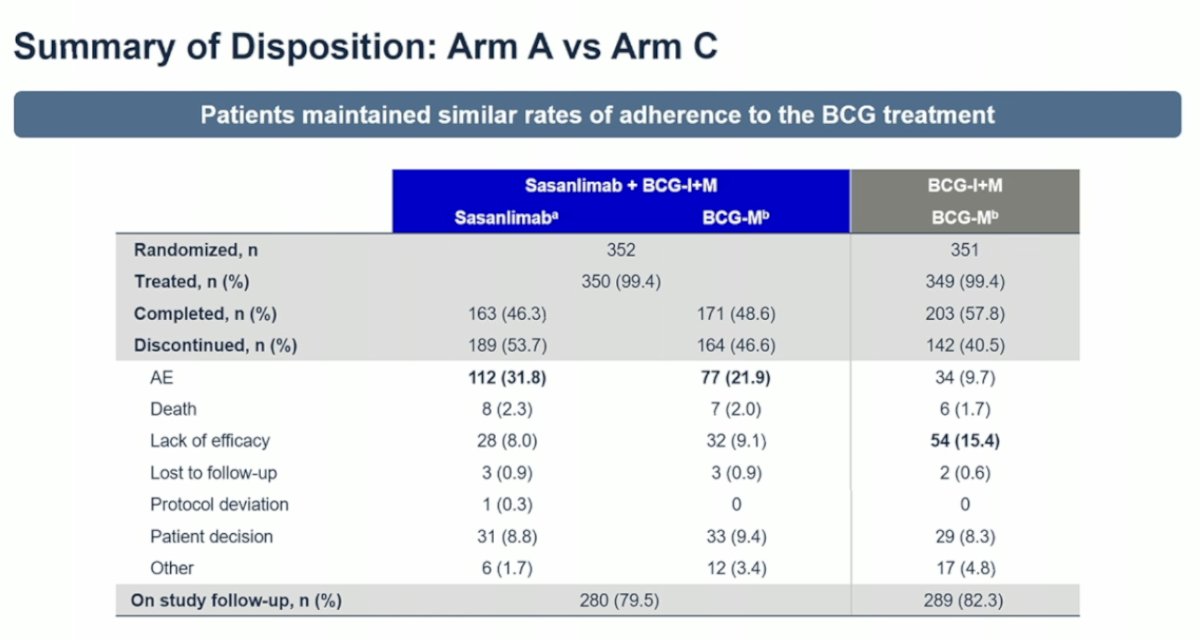
Notably, discontinuation rates were similar between the arms, with 46.6% of patients in Arm A and 40.5% in Arm C discontinuing BCG maintenance. Importantly, adherence rates were comparable, indicating that the addition of sasanlimab did not negatively impact the completion of BCG induction and maintenance therapy.
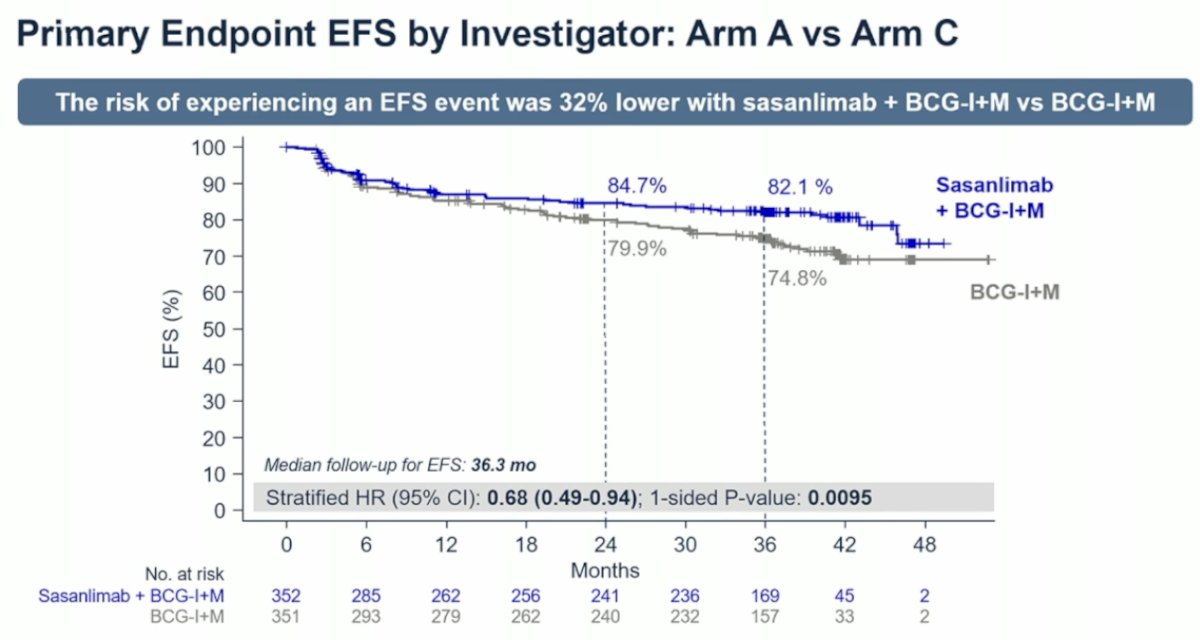
Dr. Shore highlighted that the risk of experiencing an EFS event was 32% lower with sasanlimab plus BCG compared to BCG induction and maintenance alone (stratified HR [95% CI]: 0.68 [0.49–0.94]; 1-sided P-value: 0.0095). The median follow-up for EFS was 36.3 months.
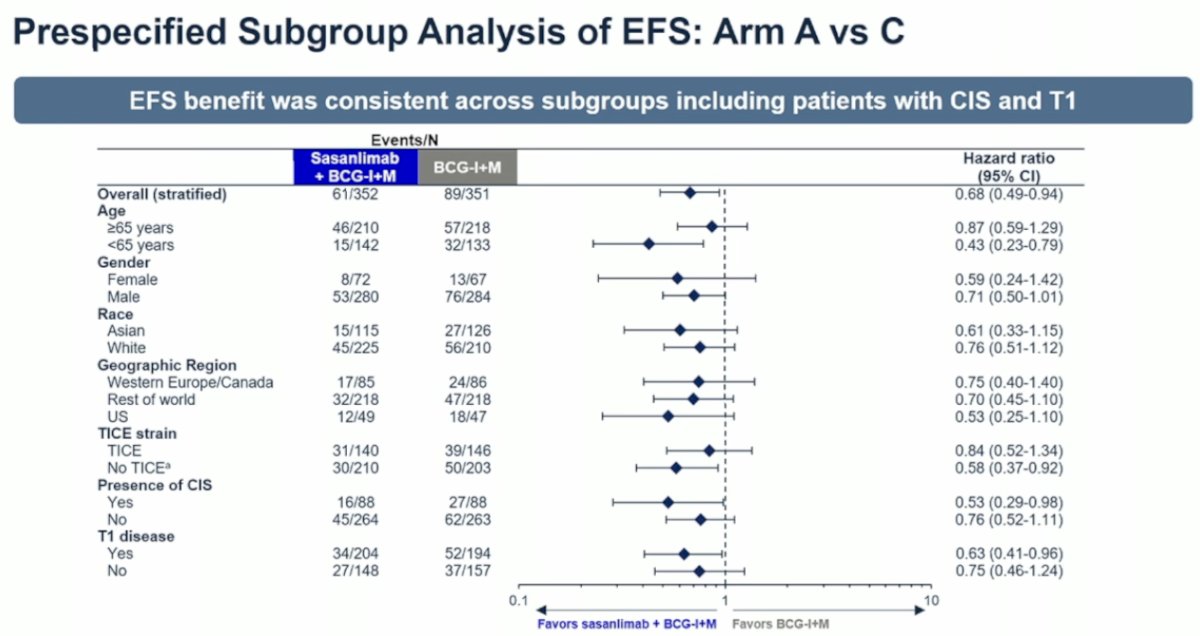
In the prespecified subgroup analysis of EFS, the benefit of sasanlimab plus BCG was consistent across subgroups, including patients with CIS and those with T1 disease. The combination treatment favored improved outcomes both in patients with the presence of CIS and in those with T1 disease.
Notably, the rate of recurrence of high-grade disease was reduced by more than 50% with sasanlimab plus BCG induction and maintenance compared to BCG induction and maintenance alone. The high-grade recurrence rates were 7.4% versus 15.1%, respectively.

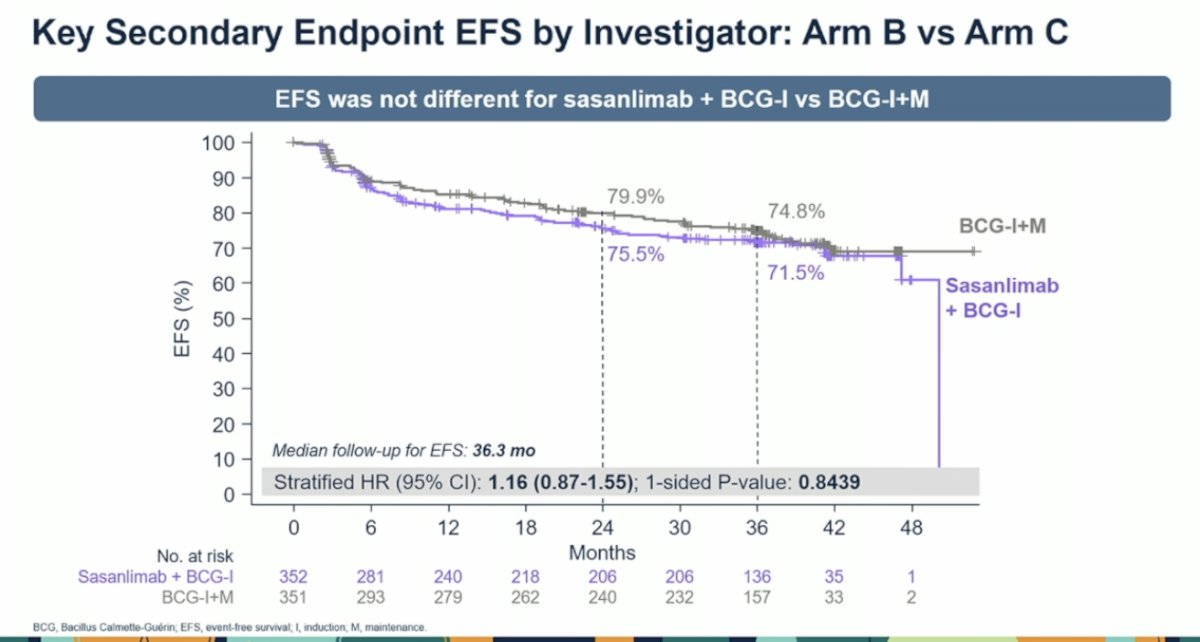
Dr. Shore highlighted that when comparing Arm B versus Arm C, EFS was not significantly different between sasanlimab plus BCG induction and BCG induction plus maintenance, underscoring the importance of BCG maintenance therapy in high-risk NMIBC.
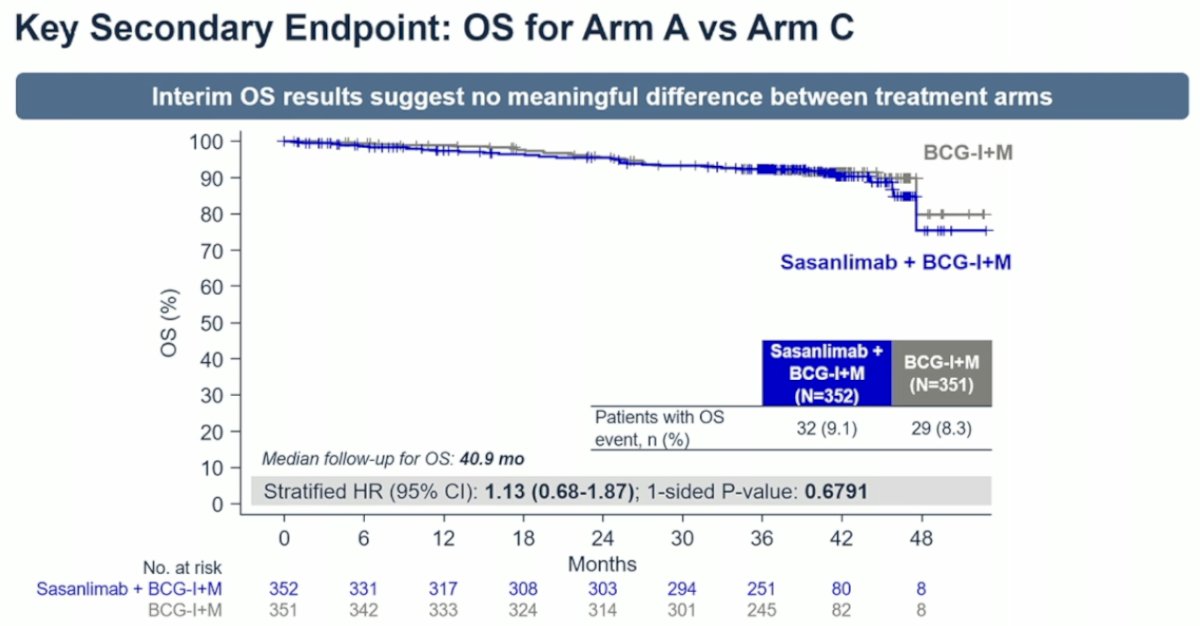
The investigators found very few cancer-related deaths. At a median follow-up of 40.9 months, overall survival (OS) events occurred in only 9.1% of patients in Arm A compared to 8.4% in Arm C, and interim OS results suggest no significant difference between treatment arms.
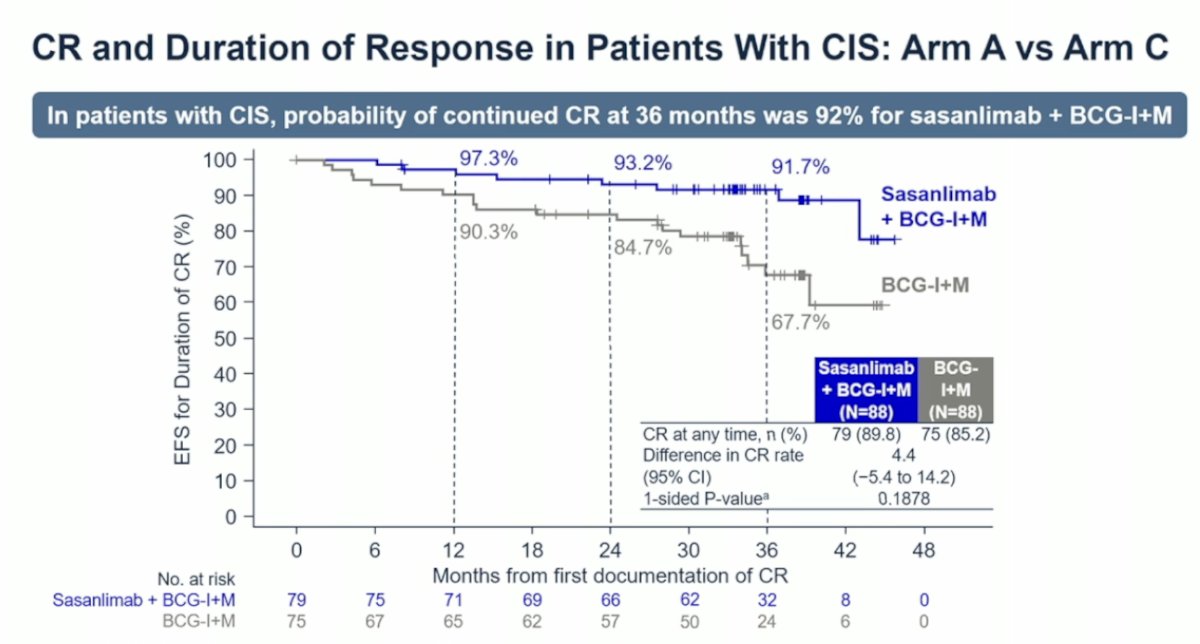
Another particularly compelling finding was that, in patients with CIS, the probability of maintaining a complete response (CR) at 36 months was 92% with sasanlimab plus BCG induction and maintenance, compared to 84.7% with BCG induction and maintenance alone.
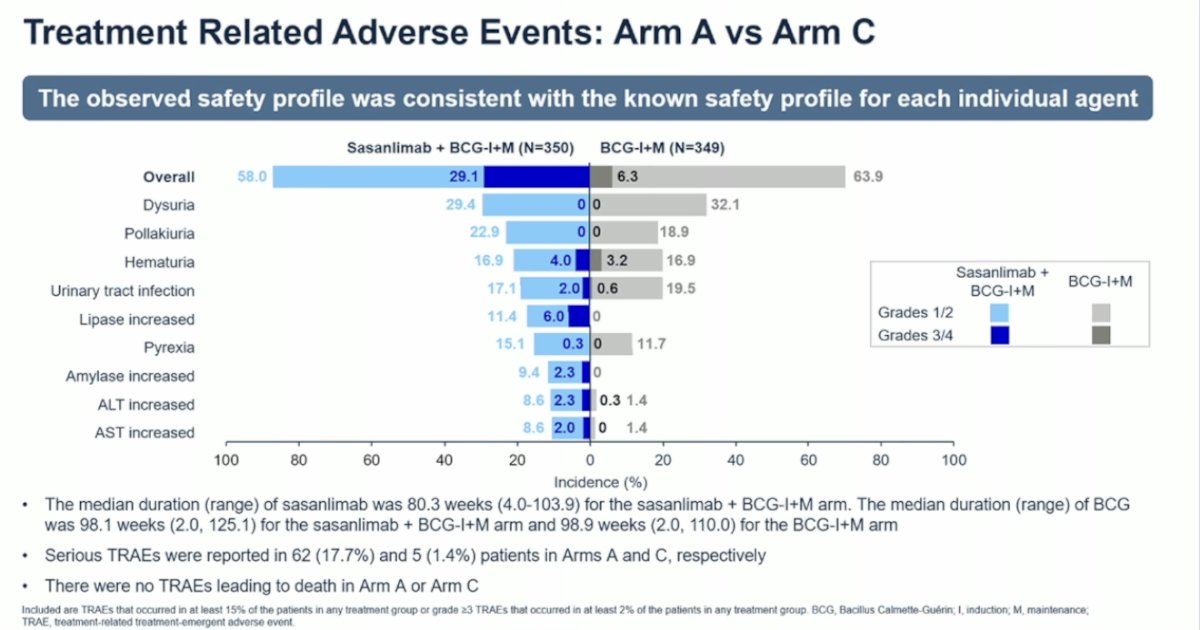
The median duration of sasanlimab treatment in the sasanlimab plus BCG induction and maintenance arm was 80.3 weeks (range: 4.0–103.9 weeks). The median duration of BCG therapy was 98.1 weeks (range: 2.0–125.1) in the sasanlimab plus BCG arm and 98.9 weeks (range: 2.0–110.0) in the BCG induction and maintenance arm. Serious treatment-related adverse events (TRAEs) were reported in 17.7% of patients (62 patients) in Arm A and 1.4% of patients (5 patients) in Arm C. Importantly, there were no TRAEs leading to death in either arm. These TRAEs are consistent with the known safety profile of both BCG and sasanlimab.
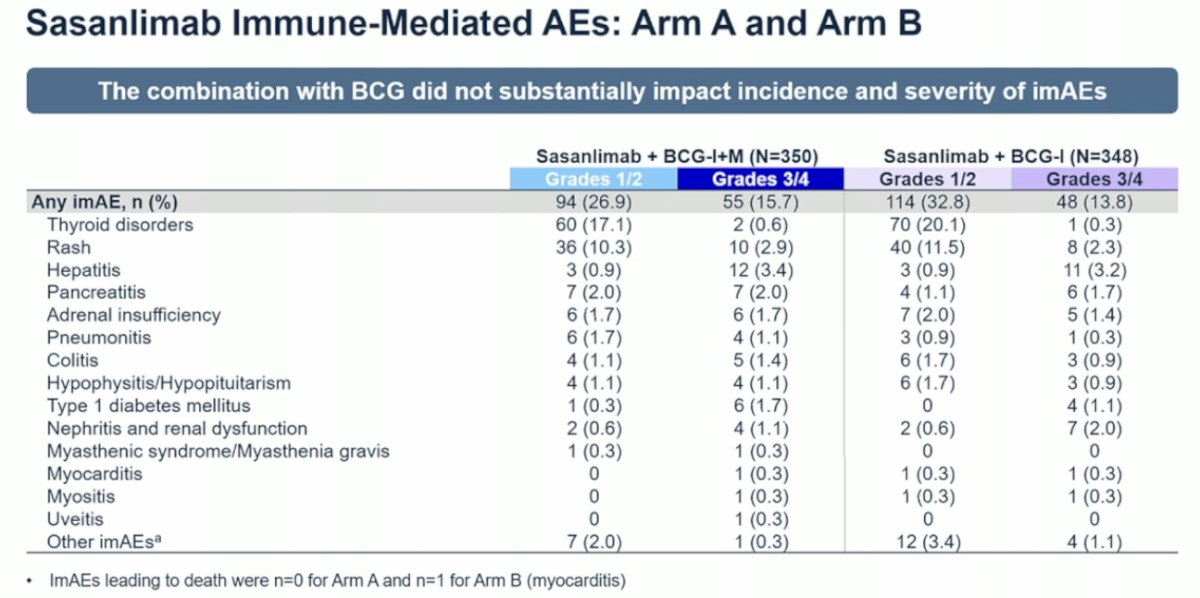
In Arm B and Arm A, which received sasanlimab, the rate of grade 3/4 adverse events was approximately 15%, with most cases resolving with thyroid hormone supplementation. All other adverse events occurred in less than 1% of patients.
Quality of life was maintained with the combination therapy, as assessed by the EORTC QLQ-C30 Global Quality of Life questionnaire.

Dr. Shore concluded the presentation with the following key messages:
- CREST is the first study showing a significant EFS benefit with sasanlimab + BCG induction and maintenance vs BCG induction and maintenance alone (HR 0.68; 95% CI: 0.49–0.94).
- In CIS patients, the probability of continued CR at 36 months was higher with sasanlimab + BCG (92% vs 68%).
- The safety profile of sasanlimab + BCG was consistent with the known profiles of each agent individually.
- Subcutaneous sasanlimab + BCG may redefine treatment for HR-NMIBC, particularly for CIS and T1 disease.
- Multidisciplinary workflows are critical for monitoring and managing imAEs.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025