(UroToday.com) On the third day of the annual World Congress of Endourology and Uro-Technology Meeting, Dr. Ahmed Ghazi, MD, MS of Johns Hopkins University delivered a State-of-the-Art Lecture Plenary on 3D printing in surgery. Over recent years, urology has witnessed a robust technological evolution, including the advancement and integration of 3D technologies.
Dr. Ghazi began by briefly reviewing the origins of 3D printing, noting that nearly thirty years have passed since Charles Hull invented stereolithography, the foundation of 3D printing. In additive manufacturing, a type of 3D printing, structures are created from ground up rather than carved away from excess material, saving both time and costs. There are a multitude of printer types, with one of the most common including fused deposition modeling (FDM). This method utilizes a filament, such as polylactic acid (PLA), which is melted and deposited layer by layer, one millimeter at a time, until the entire structure is complete. Dr. Ghazi highlighted the range of materials widely available, from flexible filaments to transparent and weight-resistant types.
He then reviewed the basic structure and function of a 3D printer. Each printer operates with several standard components: a build plate, a gantry, a filament spool feeding into a heated nozzle, and motors that move the nozzle along the x, y, and z axes. This combination allows for two-dimensional layering, while the movement of the build plate in the y-axis provides the third dimension. All 3D printers are limited by their build volume, determined by the height, width, and depth of the machine. With a computer-aided design program (CAD), digital models are exported in standard triangle language (STL) format, and further processed in a slicer program that divides the structure into layers. These layers are then converted into G-code instructions, acting as the “GPS coordinates” for the printer. Any model with an overhang greater than two centimeters requires support material, which is removed after printing.
3D printing offers a unique advantage by enabling urologic surgeons to appreciate anatomical structures that were previously only visible intraoperatively or difficult to conceptualize on flat, two-dimensional imaging. Urologic anatomy is inherently complex, as is true for the kidney, bladder, prostate, and other organs. With the predominance of minimally invasive surgery, the demand for intricate anatomical detail has only grown more critical. This need is heightened in cases of unique patient anatomy, such as tumor variability, complex stone disease, and congenital malformations. To this end, Dr. Ghazi emphasized four central applications of 3D printing in his lecture: 1) patient-specific surgical planning, 2) simulation, 3) implants and equipment, and 4) bioprinting. While there are numerous applications of 3D printing in urology, Dr. Ghazi included studies that demonstrated direct impact on patient outcomes, underscoring their clinical relevance and translational value. As outlined in Figure 1, the workflow begins with patient imaging, followed by segmentation and model generation, leading to a tangible representation of anatomy for preoperative planning.

Figure 1.
He first turned attention to surgical planning encompassed by visual aids, patient-specific 3D models, and full surgical rehearsals. In an effort to achieve realistic simulation, these models incorporate advanced techniques and materials to closely replicate human anatomy and tissue properties, requiring high-level printers and complex fabrication processes for production. A strong example of this application can be observed in patients with renal cancer undergoing laparoscopic partial nephrectomy. In a study by Fan et al., 69 patients were provided with 3D-printed visual aids for preoperative planning and compared with 58 controls. The use of 3D models resulted in differences in warm ischemia time and hospital stay, with sub analysis demonstrating reduced estimated blood loss (EBL) and improved surgeon confidence, though complication rates remained similar.1
Building upon this, Maddox et al. introduced patient-specific 3D-printed models for surgical rehearsal, enabling surgeons to practice procedures prior to live surgery. In a series of seven patients compared with a prospectively maintained cohort of 300 partial nephrectomies, benefits were observed in terms of surgical margin status and length of stay.2 Interestingly, patients in the 3D cohort experienced increased ischemia times. Surgeons also reported that models were overly dense and lacked realism, failing to adequately emulate intraoperative conditions such as tissue pliability and bleeding.
These limitations served as the foundation for subsequent innovation in the development of more realistic platforms for simulation and education. Dr. Ghazi and colleagues addressed this challenge through the use of hydrogel-based models, with the goal of replicating every step of surgery, including tissue handling, bleeding, leakage from the pelvicalyceal system, and other intraoperative events. The process begins with the segmentation of imaging in a CAD software, subsequently divided into several 3D-printed molds. These include a hilar mold, followed by medullary and cortical molds, with the tumor embedded in the cortical layer (Figure 2). The assembled construct is placed within a body cavity and surrounded by adjacent organs. Once completed, the model is brought into the operating room, the surgical robot is docked, and the procedure is rehearsed in real time, including simulated bleeding and other intraoperative challenges.
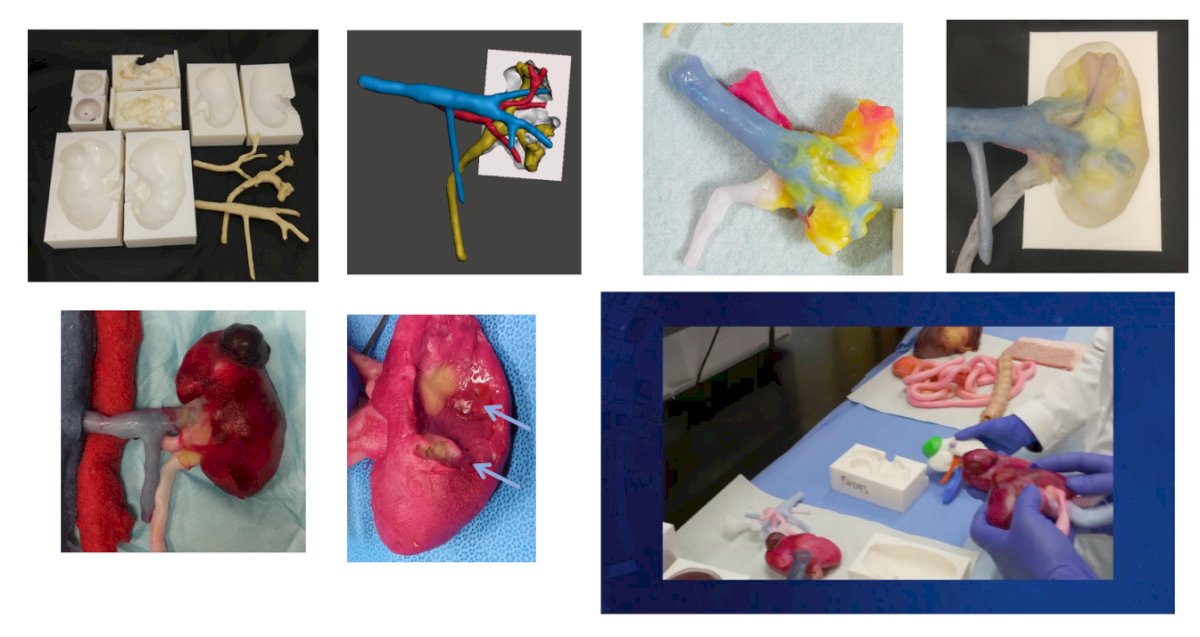
Figure 2.
Over the course of two years, Dr. Ghazi and colleagues worked aimlessly to perfect replication of properties and behavior of a cadaveric kidney. They performed rigorous testing for model validation, including both mechanical (compression, indentation, elastography) and functional (perfusion and suture closure) testing. Using 3D-printed molds and polyvinyl alcohol casting, they developed a perfused hydrogel kidney model for robot-assisted partial nephrectomy. Functional testing confirmed realistic hemostasis and parenchymal closure, supporting its utility as a high-fidelity, reproducible training platform.3 With regard to anatomical verification, they assessed the accuracy of 3D-printed, hydrogel patient-specific rehearsal models for robotic assisted partial nephrectomy and percutaneous nephrolithotomy, comparing them to patient imaging. Most structures showed deviations within 2–3 mm, supporting their reliability and underscoring the need for quality control in surgical simulation.4
They subsequently conducted a predictability study involving 20 patients across four surgeons, in which surgical planning was based on CT or axial imaging, following by rehearsal and then live surgery. A positive correlation was found between rehearsal and intraoperative performance, regardless of modality. In a second prospective study, 25 complex patients (Nephrometry score ≥8) who underwent rehearsal were compared with a matched cohort of 38 patients. While no differences were seen in warm ischemia time or blood loss, the complicate rate was reduced fivefold (Figure 3). Importantly, surgeons consistently achieved negative margins while avoiding violation of the pelvicalyceal system, enabling precise tumor excision.5 Several described the rehearsal as a “déjà vu moment,” noting that maneuvers preformed intraoperatively felt identical to those practice during rehearsal.

Figure 3.
Dr. Ghazi also highlighted randomized studies in complex endourologic cases, including staghorn stones and patients with congenital malformations. In these cohorts, 3D-printed rehearsal models improved accuracy of percutaneous access, consistency of targeting, and stone clearance rates. When initial use as rehearsal platforms showed no significant differences in complication rates or hospital stay, a subsequent randomized controlled study of 90 patients with complex renal stones and congenital malformations demonstrated significant benefits. Operative time was reduced, stone clearance rates improved, and postoperative complications were decreased,6 underscoring the value of this modality in complex cases. His group reported similar findings in percutaneous nephrolithotomy (PCNL), with decreased fluoroscopy time, fewer access attempts, fewer postoperative complications, and reduced need for secondary procedures.7
Simulation for training was another area of emphasis. Dr. Ghazi and his team developed hydrogel-based prostatectomy models derived from patient MRI data, segmented into multiple molds replicating pelvic anatomy with sensors to simulate bleeding. A bladder with multilayered structure, vascular bundles, fat, and hemostatic properties was incorporated, enabling reproduction of nearly every surgical step with high fidelity. Model performance was assessed using clinically relevant objective metrics, including positive surgical margins, leak tests, suture tension on neurovascular bundles, and operative precision, with clear differences observed between expert and novice surgeons. He further noted that single-port and multi-port robots have been successfully simulated using this platform (Figure 4).

Figure 4.
Beyond rehearsal and training, other applications include customized surgical guides for percutaneous access, prostate mapping through printed pathology slides compared with MRI correlation, and the development of custom stents. Dr. Ghazi closed this section by discussing bioprinting, which does not involve printing entire organs but instead fabricates scaffolds that support cultured cells in structured formats. Early work in pediatric bladder augmentation and animal models has demonstrated promising outcomes, with evidence of integration and function at short-term follow-up.8
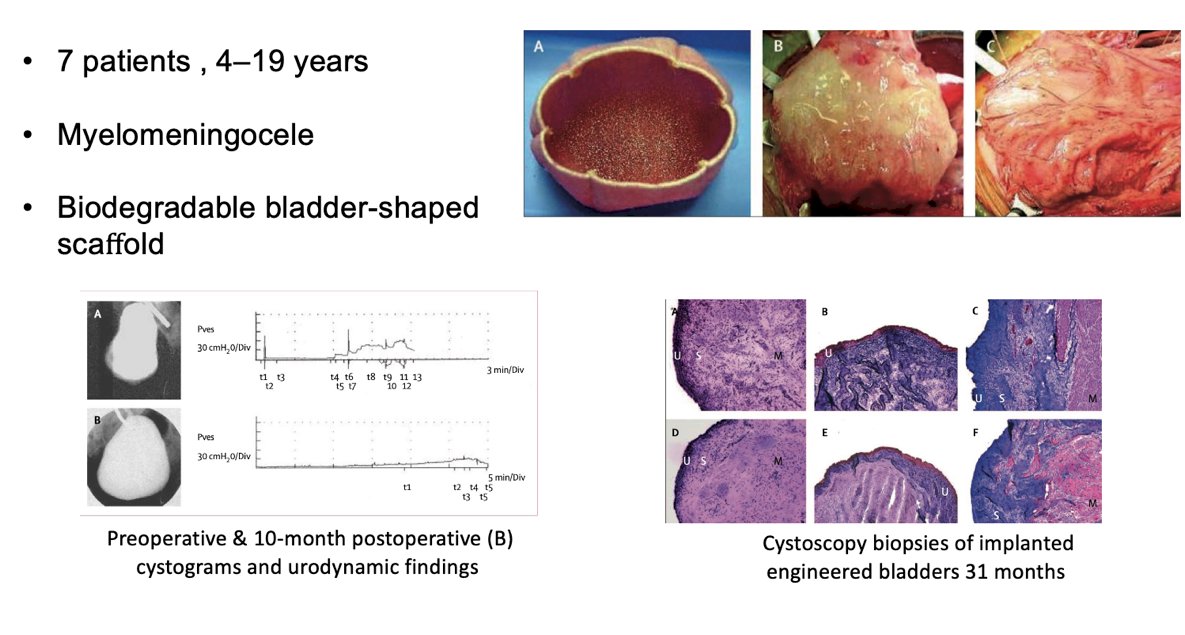
Figure 5.
In closing, Dr. Ghazi underscored that 3D printing holds immense potential to transform surgery, education, and research within urology. By enabling personalized, patient-centered models, these technologies offer surgeons the ability to plan and rehearse procedures in advance, supporting greater precision and, in complex cases, reductions in complications and improvements in outcomes. He noted that such applications represent an important step toward precision medicine, where individualized anatomic detail can guide tailored operative approaches. At the same time, he cautioned that significant challenges remain. The current body of evidence is limited, with many studies lacking adequate control arms and only demonstrating outcome improvements in select, high-complexity patients. High costs, long production times, and limited scalability restrict widespread use, while printed tools may be unsuitable for sterilization in the operating room. Despite these hurdles, Dr. Ghazi emphasized that with ongoing refinements, integration of imaging and artificial intelligence platforms, and rigorous validation, 3D printing is well positioned to become a disruptive technology that reshapes the future of urologic practice.
Presented by: Ahmed Ghazi, MD, MS, Brady Urological Institute, John Hopkins University
Written by: Mariah Hernandez, Research Specialist, Department of Urology, University of California Irvine, @mariahch00 on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Fan G, Meng Y, Zhu S, et al. Three-dimensional printing for laparoscopic partial nephrectomy in patients with renal tumors. J Int Med Res. 2019;47(9):4324-4332. doi:10.1177/0300060519862058
- Maddox MM, Feibus A, Liu J, Wang J, Thomas R, Silberstein JL. 3D-printed soft-tissue physical models of renal malignancies for individualized surgical simulation: a feasibility study. J Robot Surg. 2018;12(1):27-33. doi:10.1007/s11701-017-0680-6
- Melnyk R, Ezzat B, Belfast E, et al. Mechanical and functional validation of a perfused, robot-assisted partial nephrectomy simulation platform using a combination of 3D printing and hydrogel casting. World J Urol. 2020;38(7):1631-1641. doi:10.1007/s00345-019-02989-z
- Melnyk R, Oppenheimer D, Ghazi AE. How specific are patient-specific simulations? Analyzing the accuracy of 3D-printing and modeling to create patient-specific rehearsals for complex urological procedures. World J Urol. 2022;40(3):621-626. doi:10.1007/s00345-021-03797-0
- Ghazi A, Saba P, Shuler N, et al. Implementation of surgical rehearsal utilizing patient specific hydrogel kidney phantoms prior to complex renal cancer surgery: a pilot study. World J Urol. 2024;42(1):602. Published 2024 Oct 29. doi:10.1007/s00345-024-05301-w
- Cui D, Yan F, Yi J, et al. Efficacy and safety of 3D printing-assisted percutaneous nephrolithotomy in complex renal calculi. Sci Rep. 2022;12(1):417. Published 2022 Jan 10. doi:10.1038/s41598-021-03851-2
- Ghazi A, Melnyk R, Farooq S, et al. Validity of a patient-specific percutaneous nephrolithotomy (PCNL) simulated surgical rehearsal platform: impact on patient and surgical outcomes. World J Urol. 2022;40(3):627-637. doi:10.1007/s00345-021-03766-7
- Atala A, Bauer SB, Soker S, Yoo JJ, Retik AB. Tissue-engineered autologous bladders for patients needing cystoplasty. Lancet. 2006;367(9518):1241-1246. doi:10.1016/S0140-6736(06)68438-9