(UroToday.com) The 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting held in New Orleans, LA, was host to an Oncology Discovery and Translational session. Dr. Huipan Liu presented a first-in-human study of 225Ac-LNC1011 in patients with prostate-specific membrane antigen (PSMA) positive prostate cancer.
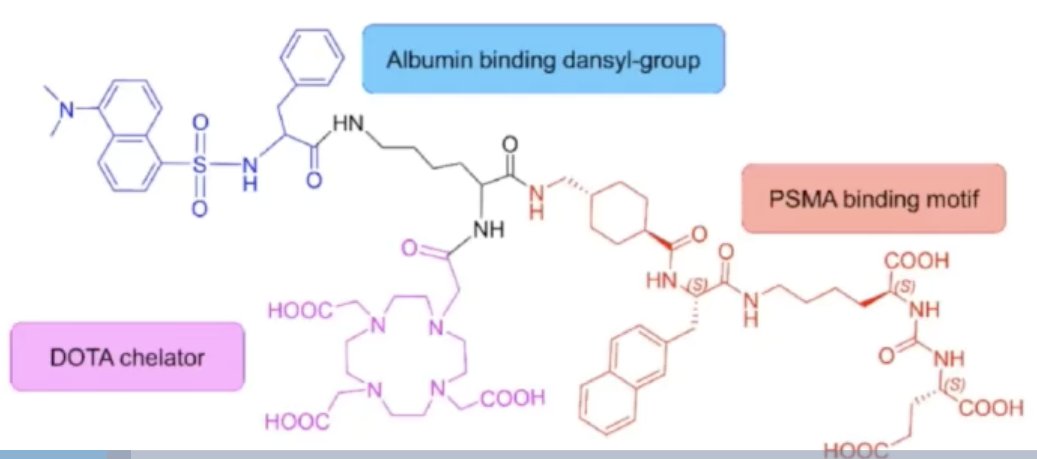
LNC1011 is a novel albumin-binding PSMA-targeting radioligand developed by LNCYT (a subsidiary of Dongcheng Pharmaceutical Group) and academic collaborators from the National University of Singapore. It incorporates a danysl amino acid linker to optimize pharmacokinetics, enhancing tumor uptake while accelerating clearance from normal organs.
Current limitations to radioligand therapy in metastatic castration-resistant prostate cancer (mCRPC) include:
- Inherent/acquired resistance to beta-emitters (~30% of patients)
- Xerostomia and hematologic toxicity with existing α-therapies (e.g., 225Ac-PSMA-617)
- Lack of agents that optimize tumor retention and organ clearance
225Ac-LNC1011’s design addresses key limitations of current PSMA radioligands by leveraging albumin binding for enhanced tumor targeting and reduced off-target toxicity, potentially establishing a new standard for α-therapy in mCRPC.
This agent includes a weak albumin-binding domain, a DOTA chelator, and a PSMA binding motif, as illustrated below:
This study aimed to evaluate the maximum tolerated dose, safety, and efficacy of 225Ac-LNC1011 targeted alpha therapy in patients with PSMA-positive prostate cancer. The study objectives were as follows:
- To assess the safety profile of 225Ac-LNC1011 (evaluated using CTCAE v.50)
- To assess the objective response rate (ORR) and progression-free survival in mCRPC patients treated with 225Ac-LNC1011
- To evaluate changes in PSA levels before and after treatment with 225Ac-LNC1011
- To evaluate changes in tumor burden SUV on 68Ga-PSMA PET/CT imaging before and after treatment with 225Ac-LNC1011
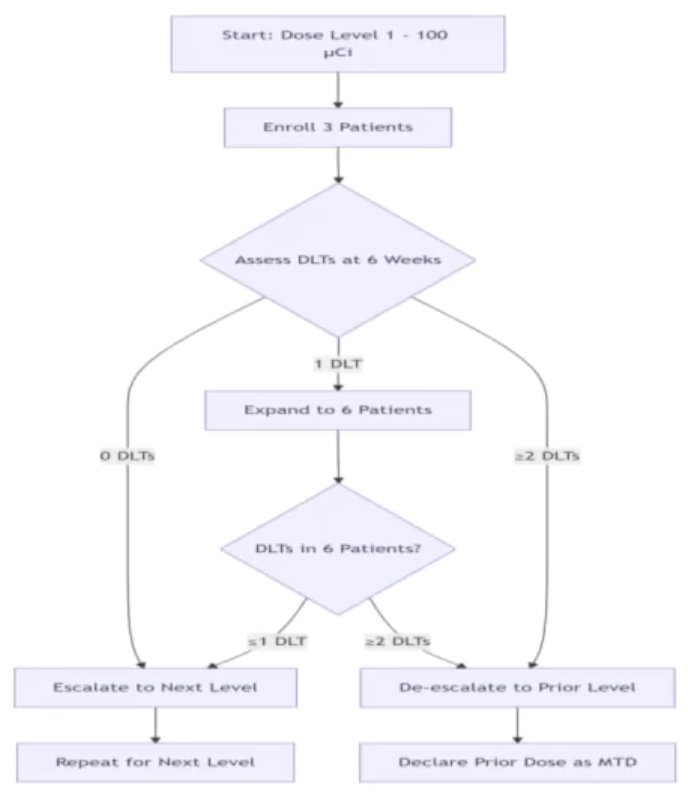
This trial followed a 3+3 dose escalation design. The initial dose was 100 µCi with 3 patients per dose level, with a maximum target dose of 200 µCi. The escalation schema was as follows:
- No dose-limiting toxicities (DLTs) in 3 patients Expand the cohort to 6 patients
- ≤1 DLT in 6 patients Escalate
- ≥2 DLTs in 3-6 patients Declare MTD reached (MTD: previous dose)
The inclusion and exclusion criteria are summarized below:

To date, 4 patients have been included, with Dr. Liu providing a detailed case presentation for each of these patients:
Patient 1: A 67-year-old man was diagnosed with mCRPC and received 177Lu-PSMA-617 treatment (2 cycles, 7.4 GBq per cycle), but experienced relapse. Before 225Ac-LNC1011 treatment, baseline 68Ga-PSMA-11 PET/CT (A) showed increased tracer uptake in the T9 adnexal region (B-C; SUVmax, 49.8; curved arrow) and the right adrenal gland (D-E; SUVmax, 2.9; long arrow). After two cycles of 225Ac-LNC1011 treatment (3.7 MBq/cycle, 9-week intervals), follow-up 68Ga-PSMA-11 PET/CT demonstrated a remarkable reduction in tracer uptake in the T9 adnexal region (G-H; SUVmax, 2.9; curved arrow). Additionally, the lesion in the right adrenal gland completely disappeared (I-J; long arrow). A biochemical response was also observed, with a decrease in serum PSA levels from 7.885 ng/mL to 0.185 ng/mL. His back pain was completely alleviated after treatment.

Patient 2: A 66-year-old man was diagnosed with mCRPC and received 225Ac-PSMA-617 treatment (2 cycles, 7.4 MBq per cycle), followed by 177Lu-PSMA-617 treatment (2 cycles, 7.4 GBq per cycle), but experienced relapse. Before 225Ac-LNC1011 treatment, baseline 68Ga-PSMA-11 PET/CT (A) revealed multiple foci of increased tracer uptake throughout the skeleton (B), particularly in the right acetabulum (C; SUVmax, 11.2; long arrow). Additionally, increased uptake was observed in a left iliac lymph node (D; SUVmax, 9.0; curved arrow). After two cycles of 225Ac-LNC1011 treatment (3.7 MBq per cycle, 9-week intervals), follow-up 68Ga-PSMA-11 PET/CT (E) showed no reduction in the number of bone lesions (F), although all lesions exhibited varying degrees of decreased tracer uptake, especially in the right acetabulum (G; SUVmax, 2.4; long arrow). Decreased uptake was also noted in the left iliac lymph node (H; SUVmax, 2.8; curved arrow). A biochemical response was observed, with serum PSA levels decreasing from 6.034 ng/mL to 1.016 ng/mL. The bone pain in the right acetabulum was significantly alleviated.

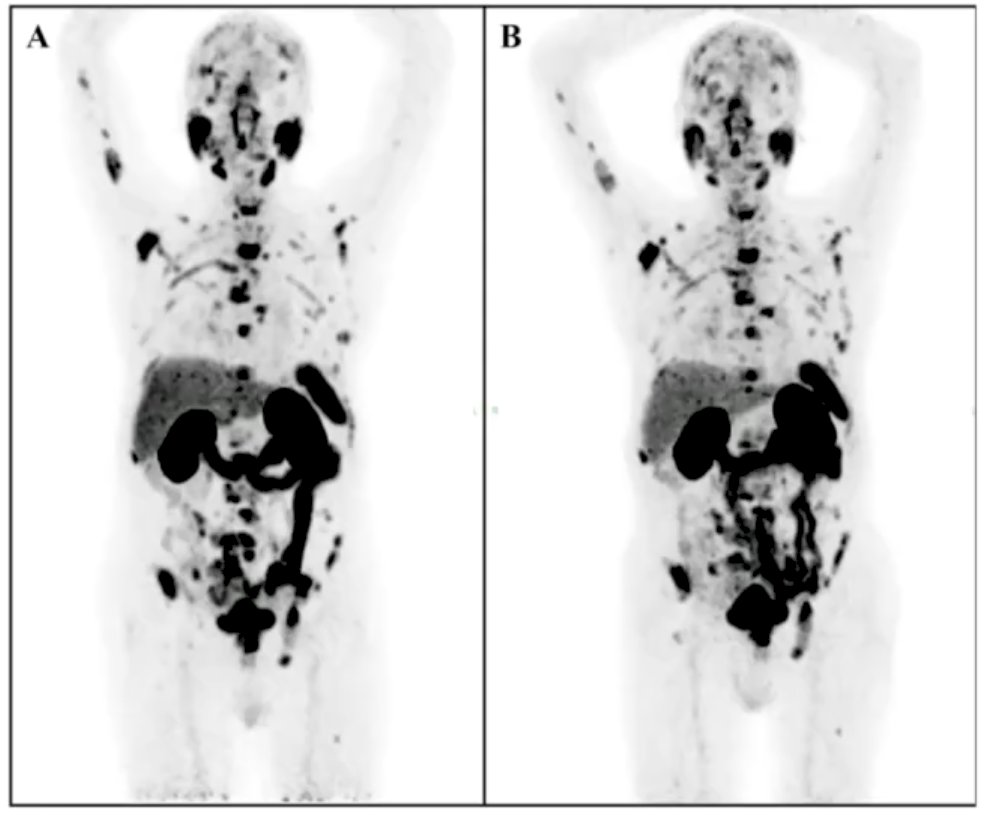
Patient 3: An 82-year-old man was diagnosed with mCRPC and received 177Lu-PSMA-617 treatment (2 cycles, 7.4 GBq per cycle), but subsequently experienced disease progression. Before 225Ac-LNC1011 treatment, baseline 68Ga-PSMA-11 PET/CT (A) revealed multiple lesions in the prostate, lymph nodes, and bones. After one cycle of 225Ac-LNC1011 treatment (3.7 MBq), follow-up 68Ga-PSMA-11 PET/CT (B) showed no significant change in tumor burden, and the patient was classified as having stable disease (SD). The serum PSA levels showed a mild decline from 353.395 ng/mL to 310.238 ng/mL. Unfortunately, the man developed a respiratory infection with progressive deterioration in his condition. He passed away in March 2025. The death was not considered directly related to the drug. Due to his baseline condition, follow-up assessments after the second treatment could not be completed, despite him having received the treatment.
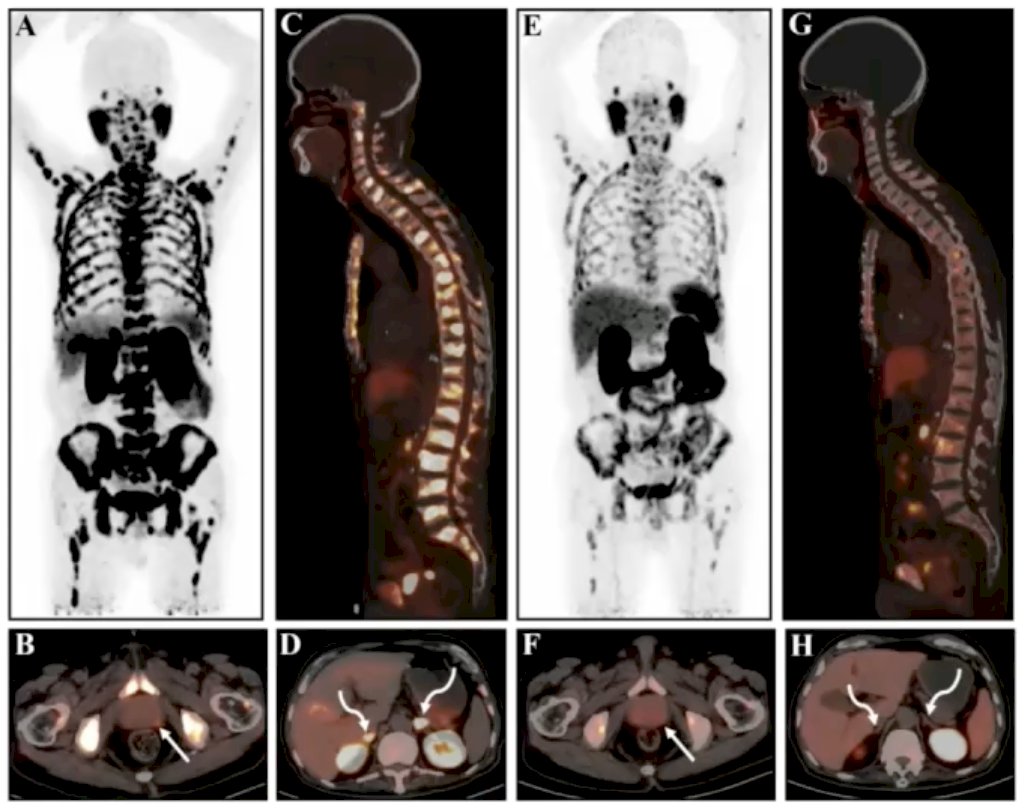
Patient 4: A 76-year-old man was diagnosed with mCRPC and received ''Lu-PSMA-617 treatment (1 cycle, 7.4 GBq per cycle). He was assessed as having stable disease (SD). Before 225Ac-LNC1011 treatment, baseline 68Ga-PSMA-11 PET/CT (A) revealed multiple lesions in the prostate (B; SUVmax, 4.1; curved arrow), bones (C; SUVmax, 28.7) and bilateral adrenal glands (D; SUVmax, 38.5; curved arrow). After two cycles of 225Ac-LNC1011 treatment (5.4 MBq/cycle, 12-week intervals), follow-up PSMA-11 PET/CT (E) demonstrated a remarkable reduction in tracer uptake in all lesions involving the prostate (F; SUVmax, 3.2; long arrow), bones (G; 12.7; curved arrow) and bilateral adrenal glands (H; SUVmax, 4.3; curved arrow). A biochemical response was also observed, with a decrease in serum PSA levels from 13.062 ng/mL to 1.057 ng/mL. His bone pain was also slightly relieved.
Overall, 2/4 patients had a RECIST 1.1 partial response resulting in an ORR of 50%. Using the PERCIST 1.0 criteria, the ORR was 75%.

The changes in PSA levels are summarized below, with 3/4 patients experiencing a PSA50 response.

Treatment-emergent adverse events were observed in 3/4 patients. All adverse events were Grade 1-2 in nature. The majority of these events were hematologic in nature (anemia, thrombocytopenia, leukopenia).

The median progression-free survival has not been reached yet.

Dr. Liu concluded that 225Ac-LNC1011 targeted-alpha therapy showed a favorable ORR and acceptable toxicity profile, making it a promising potential treatment for PSMA-positive prostate cancer. Further studies are currently underway to measure both the safety and efficacy of the treatment, as well as to determine the optimal dose and dose interval.
Presented by: Huipan Liu, MD, PhD, Department of Nuclear Medicine, The Affiliated Hospital of Southwest Medical University, PR China
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting, New Orleans, LA, June 21st – 24th, 2025