(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Dr. Aaron R. Hansen discussing results from the phase 1b TheraPb trial assessing dose escalation of 212Pb-ADVC001 in PSMA-positive metastatic castration resistant prostate cancer (mCRPC).
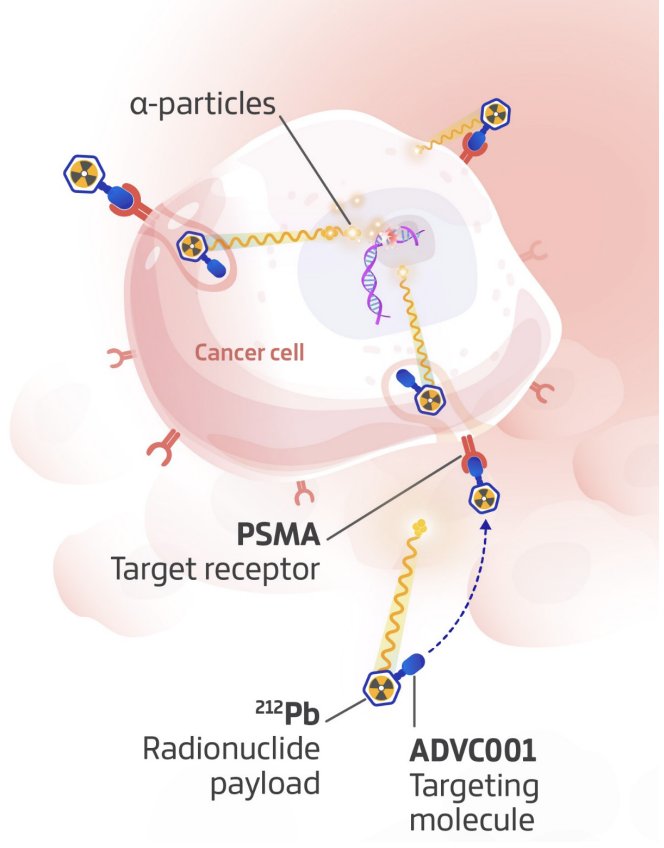
177Lu-PSMA-targeted radioligand therapy has become standard of care in mCRPC, yet ~30% of patients are resistant to 177Lu-PSMA upfront, and many who initially respond relapse during or soon after treatment.1-2 ADVC001 is a novel PSMA-targeting radioligand therapy labeled with 212Pb, an alpha-emitting payload, designed to potently kill prostate cancer cells while minimizing toxicity:
At the ESMO 2025 annual meeting, Dr. Hansen and colleagues presented the first-in-human data of 212Pb-ADVC001 in patients with mCRPC from the TheraPb trial.
This was an open-label, multi-center, interval 3+3 dose-escalation and expansion study in patients with progressive PSMA-avid (>liver) mCRPC previously treated with ≥1 androgen pathway inhibitor and ≥1 taxane unless unsuitable/declined. The primary endpoints were safety and defining the recommended phase 2 dose. Escalating doses of 60–200 MBq were administered at prespecified schedules every 6 (Cohort 1), 4 (Cohorts 2a, 3a, 4a) or 2 weeks (optional Cohorts b) for up to 6 cycles:

The primary outcome was to select the recommended phase 2 dose schedule, and secondary outcomes included safety, tolerability, maximum tolerated dose, dosimetry, and preliminary efficacy.
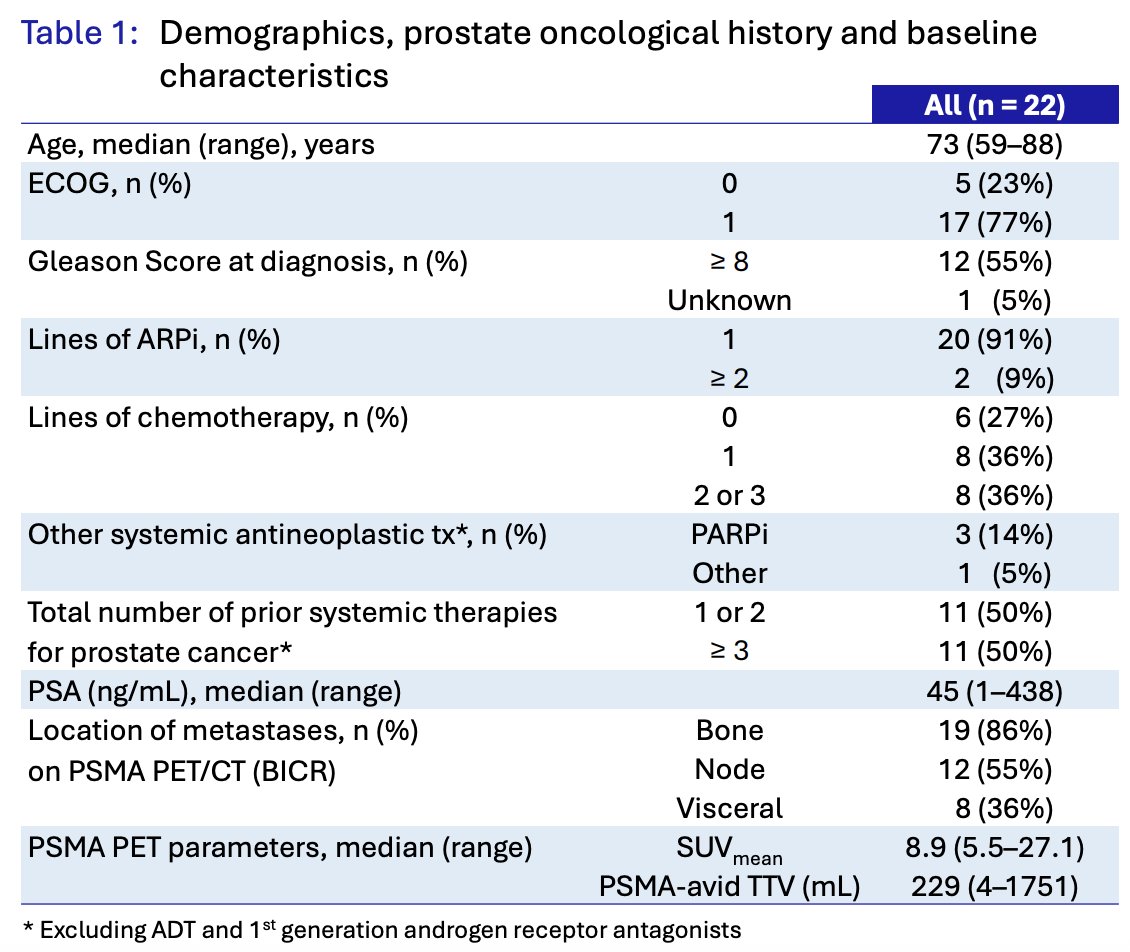
As of the cut-off of October 2, 2025, 22 patients were enrolled across 7 treatment cohorts, including 4 patients in Cohort 1 (60 MBq) and 3 patients in each subsequent cohort (120-200 MBq). The median age was 73 years (range 59–88 years), and the median PSA at baseline was 45 ng/mL (IQR 15-122). There were 73% of patients who had ≥1 prior taxane, and all had ≥1 prior androgen pathway inhibitor:
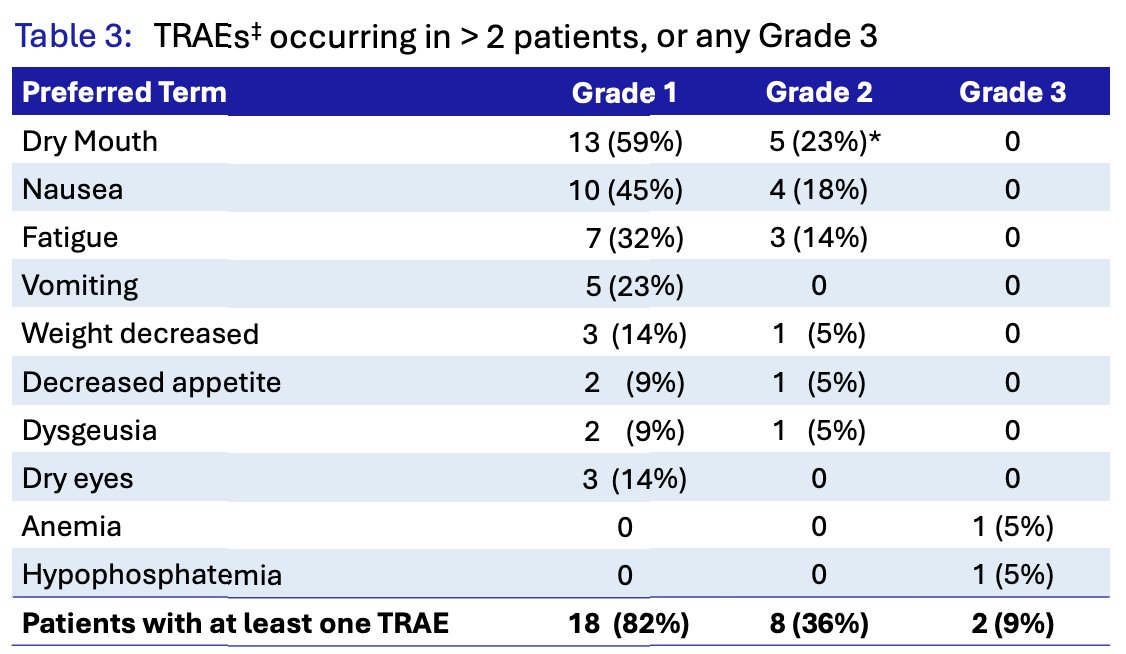
With regards to safety, there were no dose-limiting toxicities, and the maximal tolerated dose was not reached. There were also no treatment-related serious adverse events, no grade 4 treatment-emergent adverse events, and 1 unrelated grade 5 treatment-emergent adverse event 11.3 weeks after the final dose due to intracranial hemorrhage. No dose modifications or treatment discontinuations were required due to treatment-related adverse events, and 9% of patients had grade 3 treatment-related adverse events:

A 4-timepoint SPECT/CT imaging was acquired post-Cycle 1 between 1.5 and 28 hours (2.5 half-lives of 212Pb), with imaging and dosimetry analyses showing a favorable biodistribution of 212Pb-ADVC001: rapid and high uptake in tumor lesions concordant with PSMA PET, tumor retention over the decay of the isotope, fast renal clearance, and low uptake in normal organs including the salivary glands:


PSA50 was seen in 80% (12/15) of patients receiving >= 160 MBq, corresponding with decreased PSMA-avid tumor volume on PSMA PET. Additionally, 60% (9/15) of patients had a PSA80 response, and there was low upfront resistance at >= 160 MBq, with only one patient (7%) without any PSA decline. Moreover, 67% (6/9) of patients with an SUVmean <10 had a PSA50 response at >= 160 MBq:

Radiographic response per RECIST 1.1 was assessed by blinded independent central review. There were 27% of patients who had a measurable target lesion at baseline, and >=1 post-baseline imaging assessment. Overall, there was a 100% overall response rate, including 2 complete responses:

Blood and urine pharmacokinetics for 212Pb-ADVC001 showed a fast distribution and elimination, with a rapid decrease of blood concentration in the alpha phase and a beta T1/2 of ~6 hours:

Elimination was mainly through renal excretion, with a low volume of distribution (31 L) on beta phase (Vdz), suggesting limited distribution in tissues and organs. 212Pb-ADVC001 was excreted primarily in its parent form by radio-HPLC/gamma counting urine analysis, with no metabolites >= 10% of the excreted activity.
Dr. Hansen concluded his presentation discussing results from the phase 1b TheraPb trial with the following take-home points:
- ²¹²Pb-ADVC001 demonstrates encouraging safety and promising anti-tumor activity in Phase 1b
- There were no dose-limiting toxicities, treatment-related serious adverse events, or treatment-related adverse events leading to dose modification or discontinuation; xerostomia was predominantly grade 1, and evidence of reversibility
- There was an 80% PSA50 response rate at doses ≥160 MBq and a 100% overall response rate in patients with RECIST-measurable lesions, including two complete responses
- PSA, imaging, and clinical responses were frequently seen within a few weeks; a dose-effect relationship was observed, with evidence of responses in patients with baseline SUVmean < 10
- There was favorable dosimetry and kinetics with low normal organ radiation exposure that supports dosing beyond six cycles and enhanced dose intensity; there was also fast clearance and no relevant metabolic breakdown
- Phase 2 expansion will evaluate 160 MBq and 200 MBq of ²¹²Pb-ADVC001 using a randomized multi-dose-response design and adaptive dosing strategies to optimize clinical outcomes in three indications: mCRPC (chemo-naïve, and post-177Lu-PSMA) and mHSPC
Presented by: Aaron R. Hansen, BSc, MBBS, FRACP, Princess Margaret Cancer Centre, Toronto, Ontario, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.