(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a thematic session jointly organized by the Advanced Prostate Cancer Consensus Conference (APCCC) and the EAU. Dr. Karim Fizazi presented an overview of key developments in metastatic hormone-sensitive prostate cancer (mHSPC), focusing on treatment intensification strategies, emerging biomarker-driven therapy selection, and evolving phase III data across several novel therapeutic classes, including PARP inhibitors, radioligand therapy, and AKT inhibition.
Dr. Fizazi began by revisiting the role of docetaxel in the mHSPC setting, emphasizing that treatment benefit varies substantially according to disease presentation. Pooled analyses examining the effect of docetaxel on overall survival according to both metastatic burden and timing of metastatic presentation have demonstrated important heterogeneity. Among patients with low-volume metachronous disease, docetaxel was not associated with improved survival (HR: 1.13, 95% CI: 0.70–1.82; n=229).
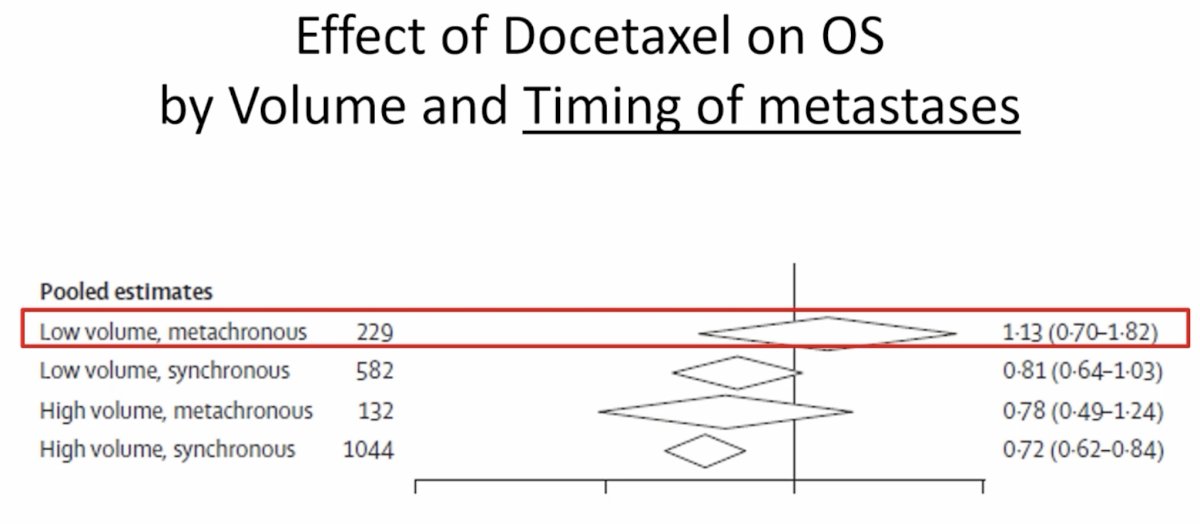
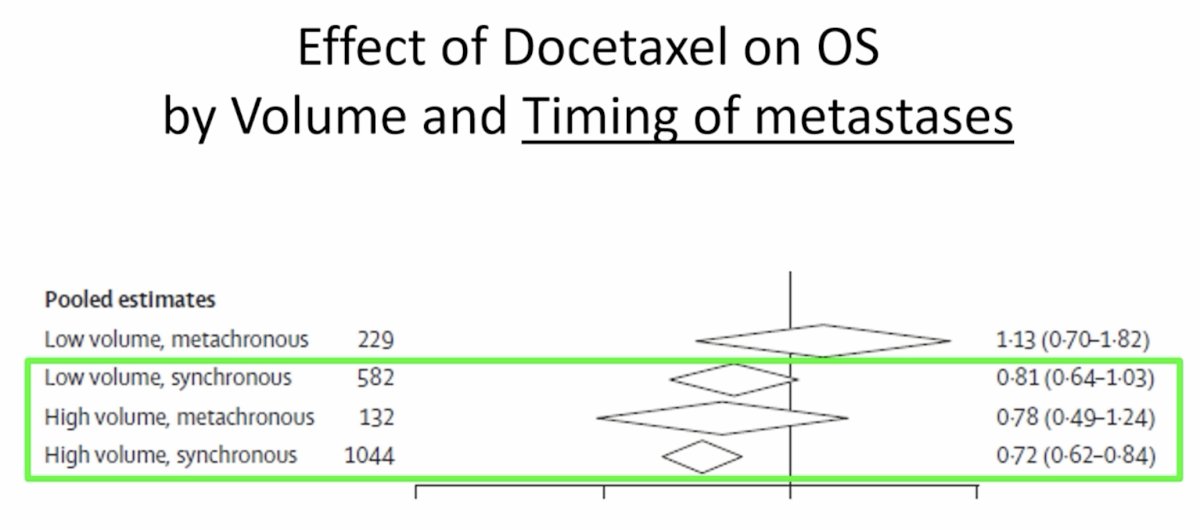
In patients with low-volume synchronous disease, the hazard ratio favored docetaxel but did not reach statistical significance (HR: 0.81, 95% CI: 0.64–1.03; n=582). Similarly, patients with high-volume metachronous disease had a numerically favorable but imprecise estimate (HR: 0.78, 95% CI: 0.49–1.24; n=132). In contrast, the clearest survival benefit was observed among patients with high-volume synchronous disease, where docetaxel significantly improved overall survival (HR: 0.72, 95% CI: 0.62–0.84; n=1,044).1 These data highlight that docetaxel provides its greatest benefit in patients presenting with de novo high-volume metastatic disease, whereas patients with metachronous relapse appear to derive less benefit from early chemotherapy intensification.
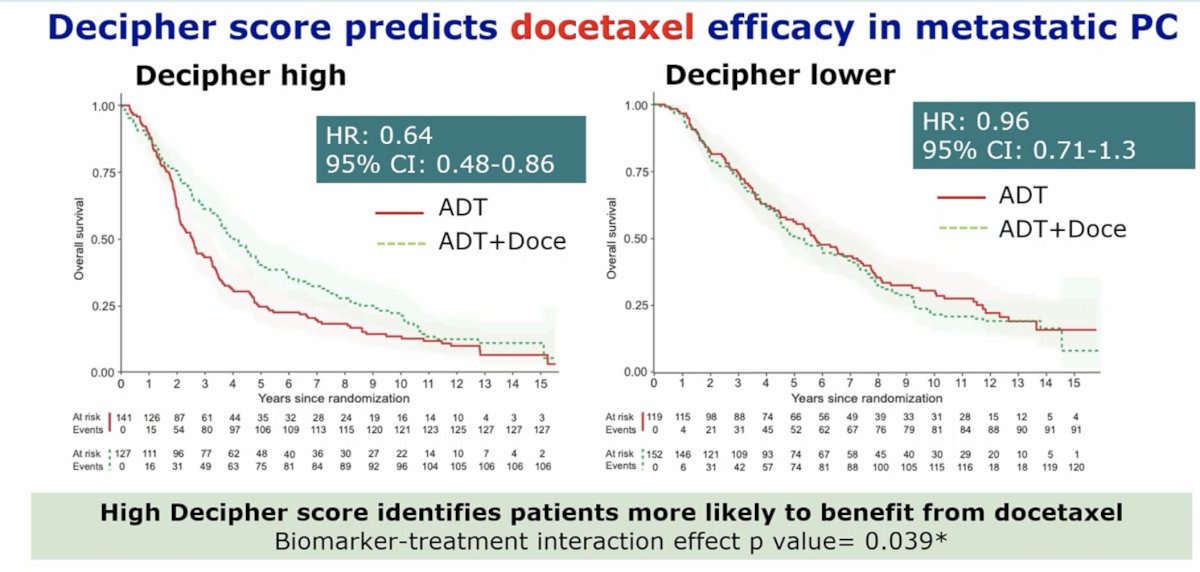
In addition to disease volume and presentation, data presented at ESMO 2024 suggest that the Decipher score may predict treatment response to docetaxel. Among patients with high Decipher scores, docetaxel significantly improved overall survival (HR: 0.64, 95% CI: 0.48–0.86), whereas no benefit was observed among those with lower Decipher scores (HR: 0.96, 95% CI: 0.71–1.30). The interaction p-value of 0.039 suggests that genomic risk may predict docetaxel benefit in mHSPC patients.
He next highlighted the importance of triplet therapy in appropriate patients using the PEACE-1 dataset. In patients treated with ADT + docetaxel, the addition of abiraterone significantly improved radiographic progression-free survival (rPFS), with a median rPFS of 4.46 years compared to 2.03 years (HR: 0.50, 99.9% CI: 0.34–0.71; p<0.0001). Overall survival (OS)was also improved, with median OS not reached in the triplet arm compared to 4.43 years with ADT + docetaxel alone (HR: 0.75, 95.1% CI: 0.59–0.95; p=0.017).2 These findings reinforce the value of systemic treatment intensification in patients with appropriate disease characteristics.
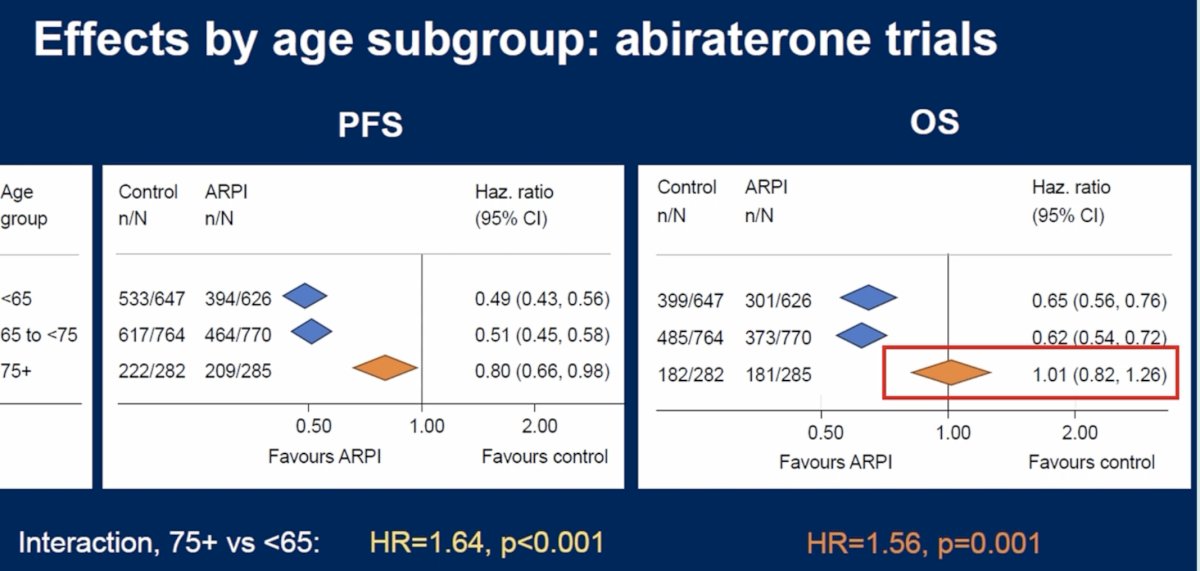
Should patient age influence androgen receptor pathway inhibitor (ARPI) selection? Analyses from abiraterone-based trials demonstrated that treatment benefit appeared attenuated among older patients. For progression-free survival, hazard ratios were 0.49 (95% CI: 0.43–0.56) for patients <65 years, 0.51 (95% CI: 0.45–0.58) for those aged 65–74 years, and 0.80 (95% CI: 0.66–0.98) among those ≥75 years. For OS, hazard ratios were 0.65 (95% CI: 0.56–0.76), 0.62 (95% CI: 0.54–0.72), and 1.01 (95% CI: 0.82–1.26), respectively, with a significant interaction for patients aged ≥75 years (interaction HR: 1.56; p=0.001). These data suggest that abiraterone may confer less benefit in the oldest subgroup.
By contrast, the “lutamide” trials evaluating enzalutamide, apalutamide, and darolutamide demonstrated consistent benefit across age strata. For progression-free survival, hazard ratios were 0.46 (95% CI: 0.39–0.55), 0.48 (95% CI: 0.42–0.55), and 0.47 (95% CI: 0.38–0.58) for patients <65, 65–74, and ≥75 years, respectively, with no interaction by age (p-value for interaction=0.88). Similarly, an OS benefit was preserved across age groups with hazard ratios of 0.61 (95% CI: 0.50–0.75), 0.69 (95% CI: 0.59–0.81), and 0.57 (95% CI: 0.45–0.71), respectively (p-value for interaction=0.61). These findings suggest that the “lutamide” class may represent a preferable ARPI strategy for patients aged ≥75 years.
Dr. Fizazi then highlighted what he described as a milestone period for precision medicine in mHSPC, beginning with the AMPLITUDE trial.3 This phase III randomized trial evaluated niraparib + abiraterone acetate and prednisone (AAP) + ADT versus placebo + AAP + ADT in patients with mHSPC harboring homologous recombination repair (HRR) gene alterations.

A total of 696 patients were randomized, and the study met its primary endpoint. Among patients with BRCA mutations, niraparib + AAP significantly improved rPFS (median not reached versus 26.0 months; HR: 0.52, 95% CI: 0.37–0.72; p<0.0001). In the overall HRR-mutated population, median rPFS was not reached with niraparib versus 29.5 months in the control arm (HR: 0.63, 95% CI: 0.49–0.80; p=0.0001). These findings represent the first positive phase III data supporting PARP inhibition in biomarker-selected mHSPC.
Radioligand therapy was the next area discussed. The PSMAddition trial evaluated the addition of 177Lu-PSMA-617 to ADT + an ARPI in patients with untreated or minimally treated mHSPC.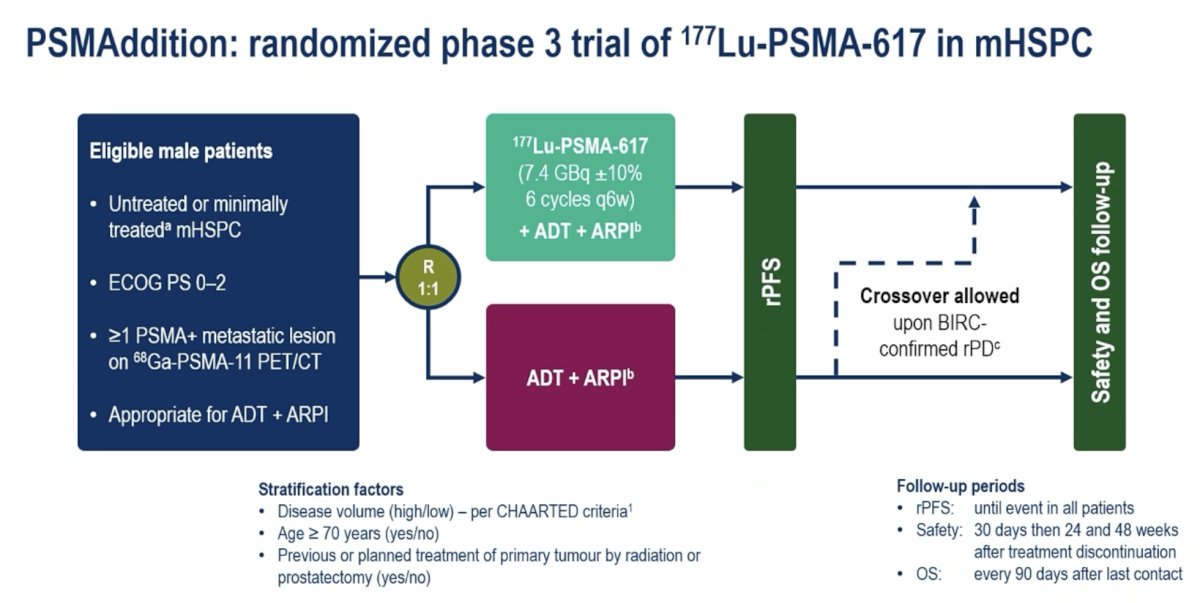
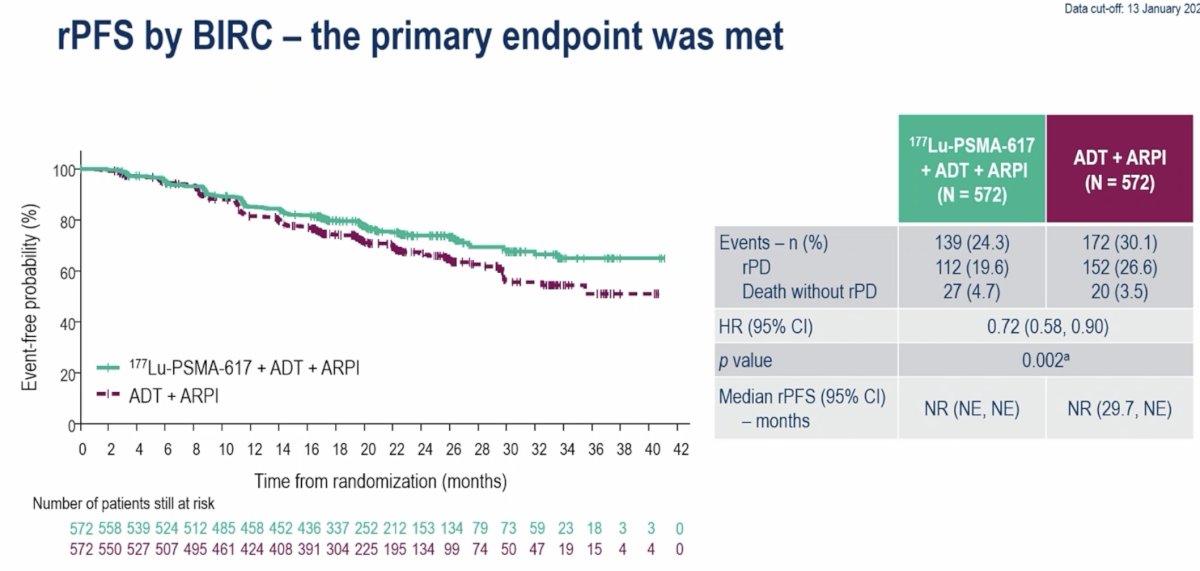
Among 572 patients per arm, the addition of radioligand therapy significantly improved rPFS, with a hazard ratio of 0.72 (95% CI: 0.58–0.90; p=0.002). Radiographic progression occurred in 19.6% of patients receiving 177Lu-PSMA-617 compared with 26.6% in the control arm. Death without prior radiographic progression occurred in 4.7% versus 3.5%, respectively. Median rPFS was not reached in either arm.
Patient-reported outcomes demonstrated no meaningful difference in time to pain worsening (HR: 1.02, 95% CI: 0.87–1.18) or time to worsening in FACT-P score (HR: 1.14, 95% CI: 0.98–1.33).
Dr. Fizazi next reviewed CAPItello-281, a randomized phase III trial evaluating the AKT inhibitor capivasertib in patients with PTEN-deficient de novo mHSPC.1 Among approximately 6,200 screened patients, 25% demonstrated PTEN deficiency and were eligible for randomization. A total of 1,012 patients were randomized to capivasertib + AAP + ADT or placebo + AAP + ADT.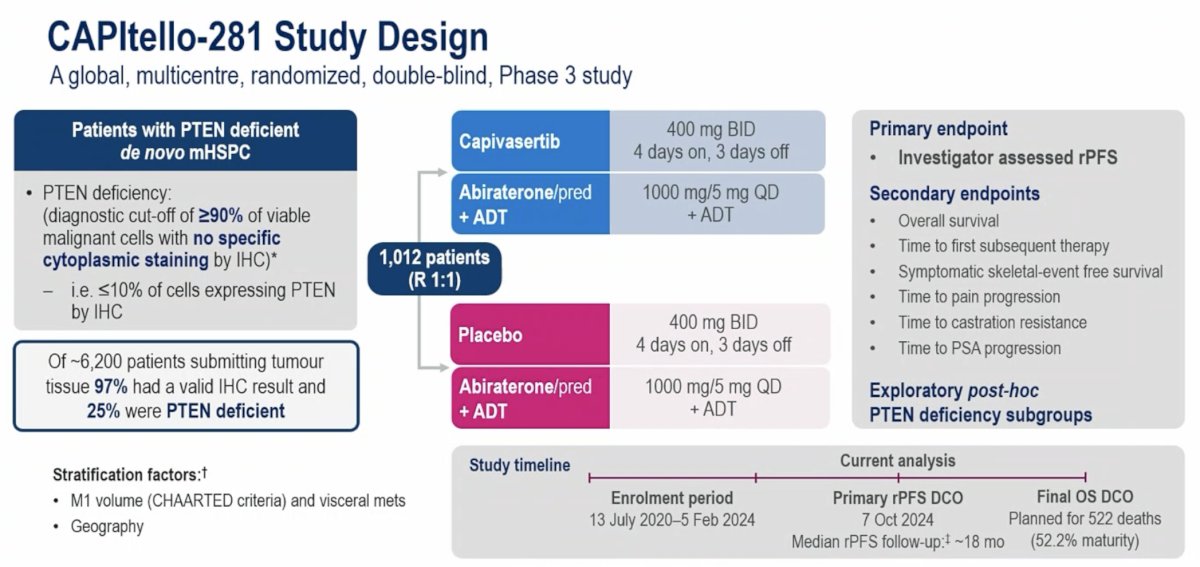
Subgroup analyses suggested that deeper PTEN loss may enrich for benefit. Using increasingly stringent definitions of PTEN loss, overall survival hazard ratios were 0.90 (95% CI: 0.71–1.15) with ≥90% PTEN loss, 0.80 (95% CI: 0.62–1.04) with ≥95% loss, 0.77 (95% CI: 0.53–1.12) with ≥99% loss, and 0.77 (95% CI: 0.51–1.14) with complete PTEN loss, suggesting that stronger biologic selection may help identify patients most likely to benefit from AKT inhibition.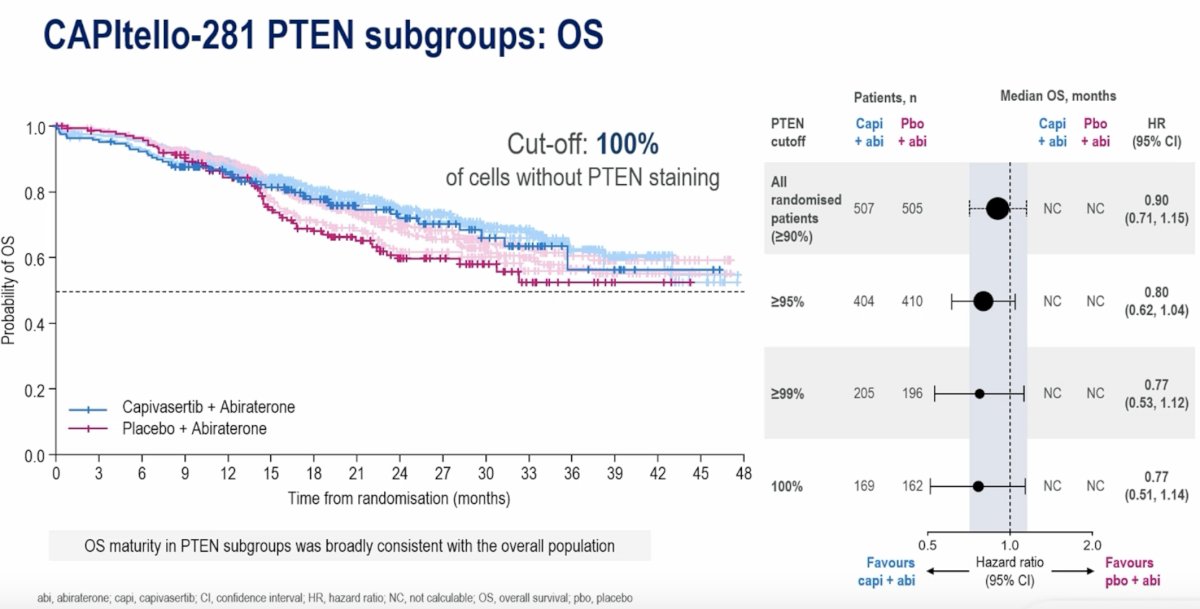
What should we expect in 2026 and beyond for mHSPC? Dr. Fizazi highlighted the TALAPRO-3 trial, which is evaluating talazoparib + enzalutamide versus placebo + enzalutamide in patients with mHSPC harboring HRR gene alterations. Eligible patients include those with alterations in ATM, ATR, BRCA1, BRCA2, CDK12, CHEK2, FANCA, MLH1, MRE11A, NBN, PALB2, or RAD51C. The primary endpoint is rPFS, with key secondary endpoints including OS, objective response rate, duration of response, and patient-reported outcomes.

Dr. Fizazi also emphasized the prognostic value of early PSA response. Data from PEACE-1 demonstrated that PSA measured at 8 months strongly stratifies OS outcomes. Among patients receiving ADT with or without docetaxel, those achieving PSA ≤0.2 ng/mL at 8 months had a median OS that was not reached (95% CI: 4.8 years to not estimable), whereas those with PSA >0.2 ng/mL had a median overall survival of 3.5 years (95% CI: 3.1–4.1; p<0.0001). Similar findings were observed among patients receiving ADT + abiraterone-based therapy, where median OS was not reached for patients with PSA ≤0.2 ng/mL compared to 3.4 years (95% CI: 2.8–3.9) for those with PSA >0.2 ng/mL (p<0.0001). These findings provide a strong rationale for response-adapted treatment strategies.

These concepts are currently being explored within the PEACE-6 program, which is evaluating response-adapted intensification strategies in mHSPC. Patients demonstrating poor PSA responses at 6–8 months are randomized to additional treatment intensification such as Lu-PSMA therapy, whereas those with excellent responses may undergo treatment de-escalation strategies.


Dr. Fizazi concluded his presentation by summarizing how the field is evolving. Historically, the key principles in de novo mHSPC included systemic treatment intensification with two or three drugs and the use of prostate radiotherapy primarily to prevent local progression without clear OS benefit in the era of modern systemic therapy. Importantly, these benefits appeared independent of metastatic burden, reinforcing the notion that clinicians should move beyond rigid volume-based treatment decisions.
Looking ahead to 2026 and beyond, several important themes are emerging. Age may increasingly influence ARPI selection, with abiraterone potentially avoided in patients older than 75 years. Biology will also play an increasingly important role in treatment selection. PARP inhibitors will likely be incorporated for patients with BRCA alterations, the role of Lu-PSMA may depend on PSMA expression and disease characteristics, and AKT inhibition with agents such as capivasertib may be particularly relevant in patients with strong PTEN deficiency. Finally, response-adapted treatment strategies—where poor responders undergo further treatment intensification and excellent responders undergo treatment de-escalation—represent a promising future direction for individualized mHSPC care.
Presented by: Karim Fizazi, MD, PhD, Professor, University of Paris Saclay, President of GETUG, Head of the Genito-Urinary Group, Department of Cancer Medicine, Institut Gustave Roussy and Centre Oscar Lambret, Villejuif, France, Institute Gustave Roussy (IGR), Villejuif, France
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the EAU 2026 Annual Congress, London, UK, March 13th–16th, 2026
- Vale CL, Fisher DJ, Godolphin PJ, et al. Which patients with metastatic hormone-sensitive prostate cancer benefit from docetaxel: a systematic review and meta-analysis of individual participant data from randomised trials. Lancet Oncol. 2023; 24(7):783-97.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022;399(10336):1695-1707.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: a randomized phase 3 trial. Nature. 2025; 31:4109-18.
- Fizazi K, Clarke NW, De Santis M, et al. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study. Annal Oncol. 2026;37(1):53-68.