(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain, between March 21st and 24th 2025, was host to a thematic session on hot topics in the management of renal cell carcinoma (RCC) patients. Dr. Axel Bex discussed neoadjuvant strategies in locally advanced RCC.
There is strong biologic and clinical rationale for neoadjuvant immunotherapy, which has demonstrated clinical benefit for patients with melanoma, as well as colorectal and bladder cancers. The presence of the tumor in situ in the neoadjuvant setting allows for clonal expansion, theoretically enhancing the potency of the immune response.

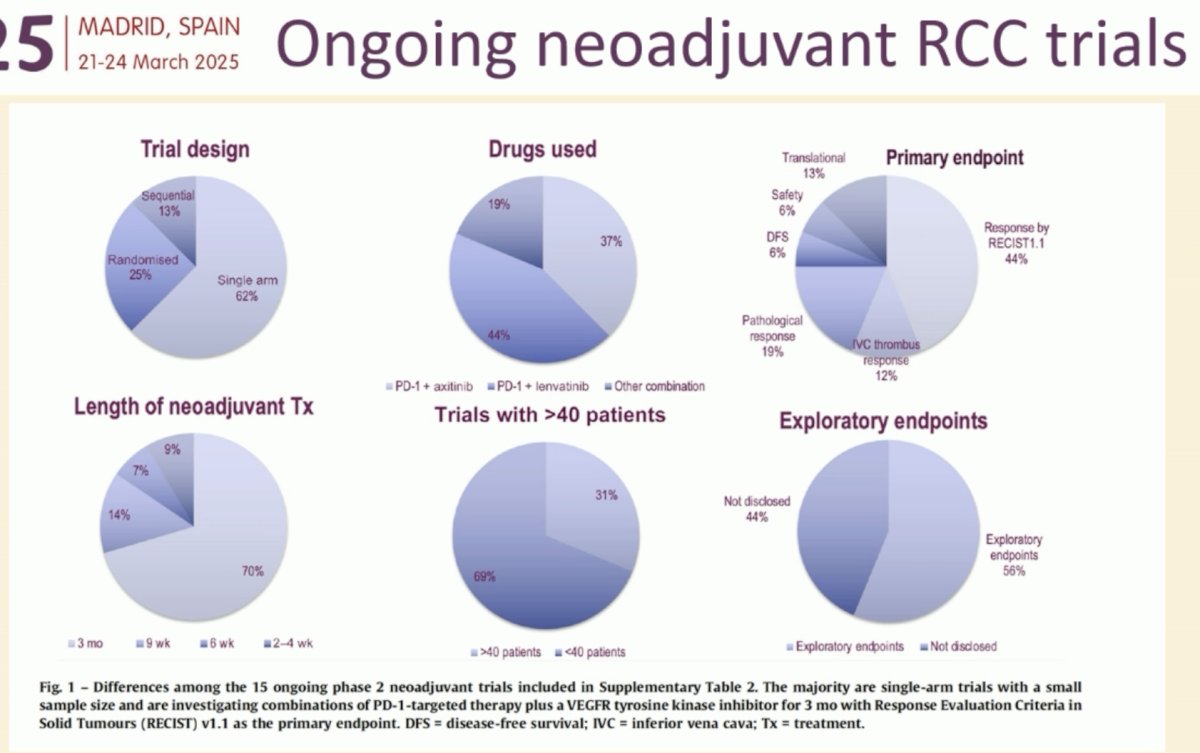
What is the current state of ongoing neoadjuvant RCC trials? In short, disappointing. The majority of ongoing trials are limited by their single arm nature (62%), small sample sizes (<40 patients: 69%), heterogeneity with regard to the drugs being evaluated, and short durations neoadjuvant therapy (≤3 months: 70%).1
The only phase III perioperative trial in RCC remains PROSPER, an open label, randomized, phase III trial that included previously untreated ≥cT2 or TanyN+ clear cell or non-clear cell RCC patients planned for partial or radical nephrectomy. Patients were randomized to either:
- Nivolumab plus surgery
- 1 dose of nivolumab pre-operatively, followed by 9 adjuvant doses (480 mg IV every 4 weeks)
- Surgery only followed by surveillance.
This trial failed to demonstrate a survival benefit with this peri-operative approach. Notably, Dr. Bex highlighted that 10-15% of the patients in both arms failed prior to surgery and had disease progression prior to undergoing surgery.2 This is reflected in the Kaplan Meier curve below, whereby the two curves do not start at 100%, reflecting the occurrence of these events prior to their partial or radical nephrectomy (i.e., T0). This is in contrast to adjuvant trials, including KEYNOTE 564, whereby patients were required to have a post-operative window where no events happened.
Dr. Bex emphasized that we have clearly lagged in the neoadjuvant/perioperative RCC space, particularly when compared to our counterparts in the melanoma disease space, where numerous international consortiums and trials have been conducted.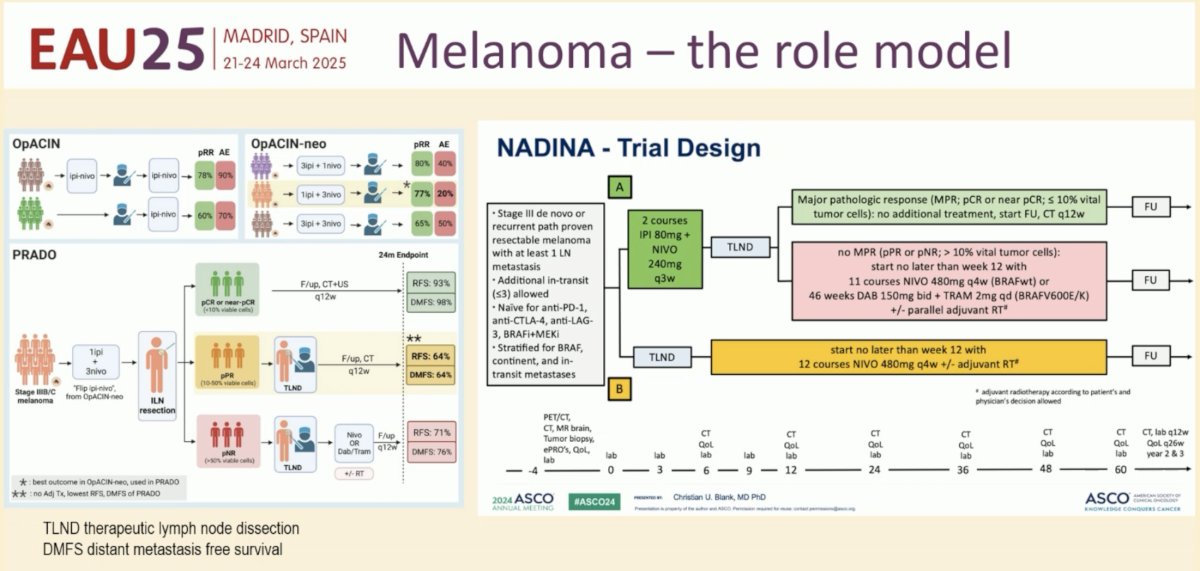
In an attempt to overcome these shortcomings, Dr. Bex and colleagues led consensus meetings in Boston and Amsterdam in 2024, engaging patient advocacy groups, in an attempt to address the following questions:
- What is the best efficacy marker to guide adaptive treatment decisions?
- What is the optimal drug or combination?
- What is the optimal length of neoadjuvant treatment?
- How to select the right patients?
- Can we agree on adaptive and practice-changing neoadjuvant trial designs?

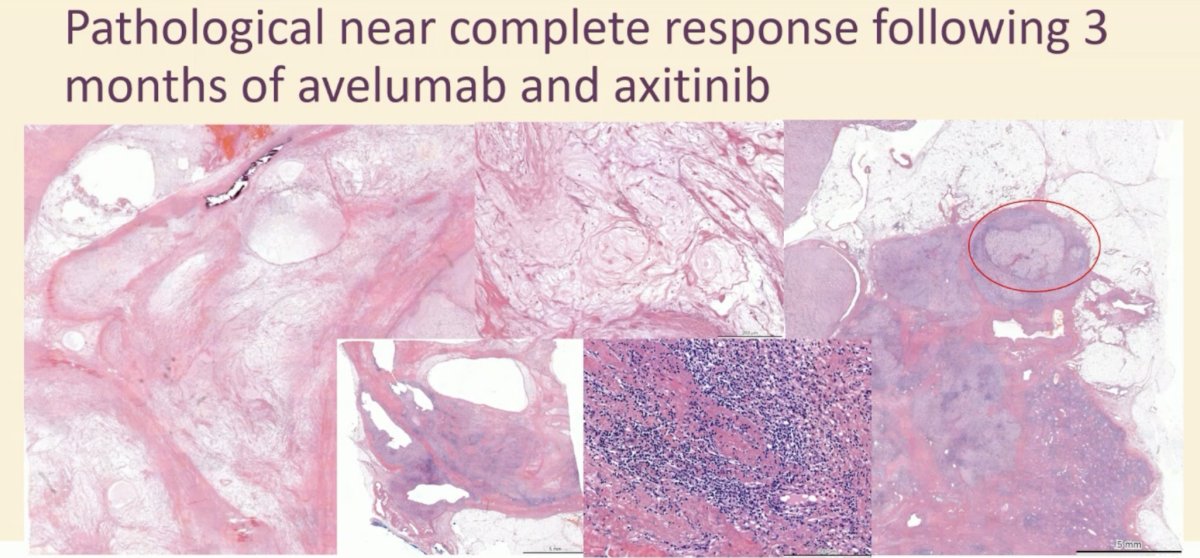
What are some other notable trials of peri-operative therapy for high-risk RCC? The NeoAvAx trial evaluated the neoadjuvant use of a combination of the immune checkpoint inhibitor avelumab and the VEGF-inhibitor axitinib (NCT03341845). This was a single arm phase II trial of adult patients with clinically high-risk clear cell RCC (cT1b-2a + G4; cT2b-3a + G3-4; cT3-4 + any grade; resectable node-positive disease) who received 12 weeks of neoadjuvant avelumab and axitinib prior to nephrectomy.
Between May 2018 and October 2021, 40 patients were enrolled. Twelve patients (30%) had a partial response of the primary tumor. The median primary tumor downsizing was 20% (+3.8 to -43.5%). No patient had a primary tumor progression, per RECIST v1.1.
Among the 12 patients with a partial response of the primary tumor, 10 (83%) were disease-free. At a median follow-up of 23.5 months, recurrence occurred in 13 (32%) patients at a median of 8 months, and 3 died of disease. Neither median disease-free survival nor overall survival has been reached to date.3
The NESCIO trial is a randomized, open-label, three-arm phase II trial that aims to assess the efficacy and safety of neoadjuvant nivolumab alone or in combination in intermediate- to high-risk non-metastatic clear cell RCC using an adaptive trial design. A maximum number of 69 patients will be randomized to receive the following therapy every 3 weeks prior to surgery:
- 2 courses of nivolumab 360 mg
- 2 courses of ipilimumab 1 mg/kg + nivolumab 3 mg/kg
- 2 courses of nivolumab 360 mg + relatlimab 360 mg
The primary endpoint is pathologic response rate, defined as the proportion of patients demonstrating a complete or partial pathologic response. Secondary endpoints include:
- Safety
- Objective response rate
- Recurrence-free survival
- Event-free survival
- Rate of distant metastases and local recurrences
- Surgical morbidity.
After 42 patients have been recruited (14 per arm), an interim analysis will be performed to evaluate the observed efficacy and toxicity within each arm and either allow for early discontinuation or continuing recruitment in the second stage of a Simon’s two stage design. The first patient was enrolled in April 2022.4
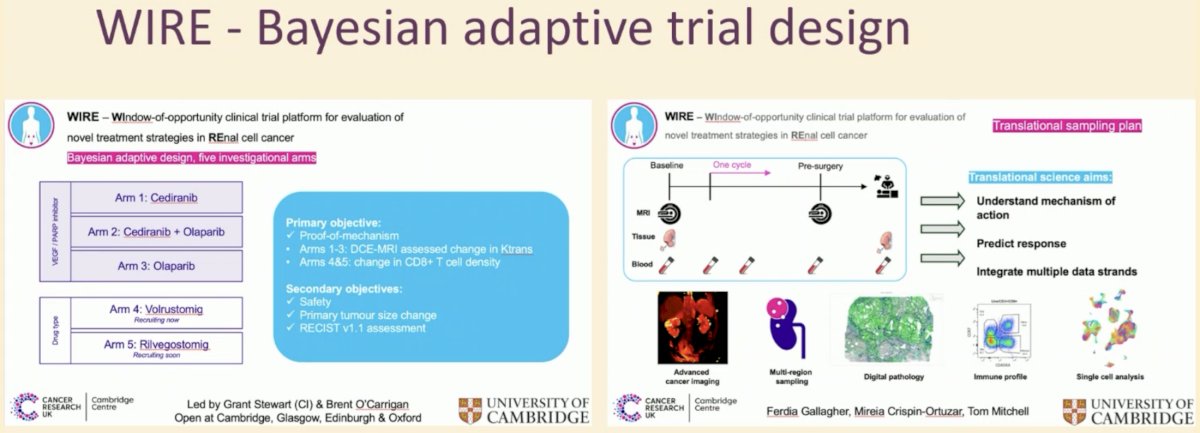
WIRE is a phase II, multi-arm, non-randomised, proof-of-mechanism platform trial using a Bayesian adaptive design. The Bayesian adaptive design leverages outcome information from initial participants during pre-specified interim analyses to determine and minimise the number of participants required to demonstrate efficacy or futility. Patients with biopsy-proven, surgically resectable, cT1b+, cN0-1, cM0-1 clear cell RCC and no contraindications to the drugs are eligible to participate.
Participants undergo diagnostic staging CT and renal mass biopsy, followed by treatment in one of the treatment arms for ≥14 days. The trial includes five treatment arms:
- Arm 1: Cediranib
- Arm 2: Cediranib + Olaparib
- Arm 3: Olaparib
- Arm 4: Volrustomig
- Arm 5: Rilvegostomig
The primary objectives are:
- Proof-of-mechanism
- Arms 1-3: DCE-MRI assessed changes in Ktrans
- Arms 4-5: Change in CD8+ T cell density5
Dr. Bex shared his ‘vision’ for the treatment of high-risk RCC, both in the neoadjuvant and adjuvant settings. In the neoadjuvant setting, high-risk patients would receive neoadjuvant therapy for 6–8 weeks, after which therapy would be tailored based on pathologic response, as summarized below:
The CARE-2 trial is a randomized neoadjuvant phase II trial of pembrolizumab + belzutifan +/- lenvatinib. Eligible high-risk RCC patients will undergo 1:1:1 randomization to:
- Pembrolizumab + lenvatinib + belzutifan x 12 weeks Nephrectomy Pembrolizumab x 9 months
- Pembrolizumab + belzutifan x 12 weeks, Nephrectomy, Pembrolizumab x 9 months
- Nephrectomy Pembrolizumab x 12 months (‘standard of care’)
The primary endpoint is the overall response rate in the primary tumor.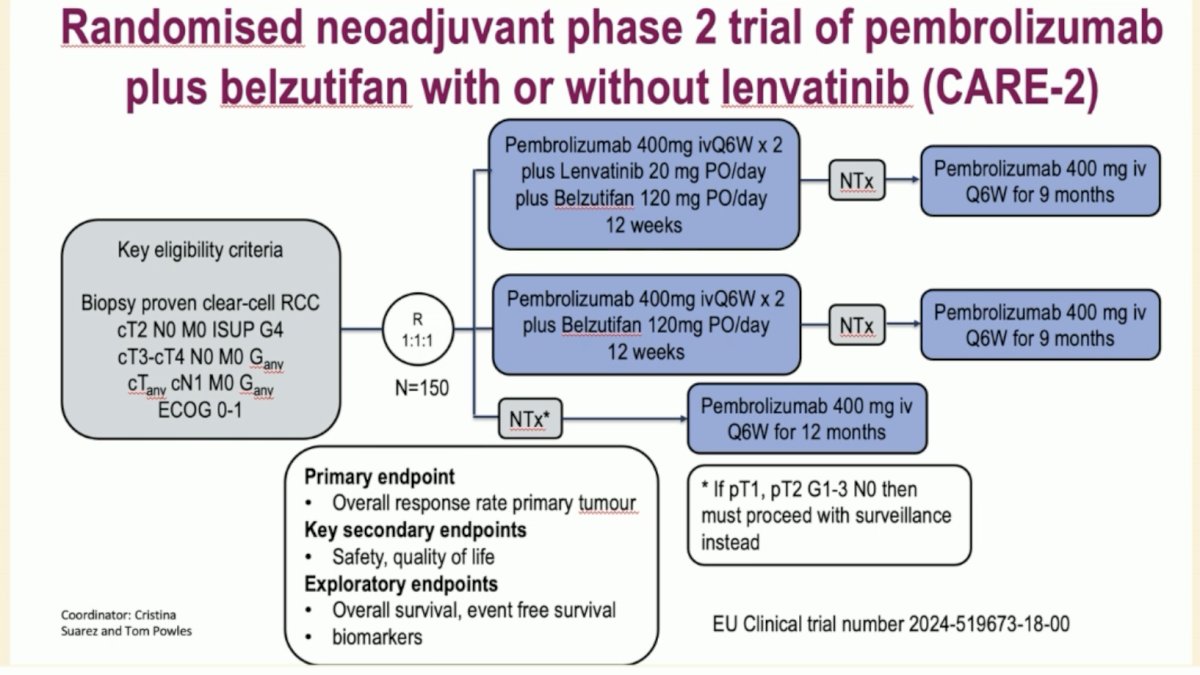
Dr. Bex concluded as follows:
- In comparison to other solid tumor types, research into neoadjuvant and perioperative strategies in RCC is fractionated and confined to small single arm studies
- International collaboration is required to harmonize research questions and translational endpoints
- Adaptive randomized platform trials are needed to develop optimal strategies, including treatment intensification or de-escalation, and randomization against the standard of care
Presented by: Axel Bex, MD, PhD, University College London, London, United Kingdom
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:- Bex A, Jewett M, Lewis B, et al. A Call for a Neoadjuvant Kidney Cancer Consortium: Lessons Learned from Other Cancer Types. Eur Urol. 2025; 87(4): 385-9.
- Allaf ME, Kim SE, Master V, et al. Perioperative nivolumab versus observation in patients with renal cell carcinoma undergoing nephrectomy (PROSPER ECOG-ACRIN EA8143): an open-label, randomised, phase 3 study. Lancet Oncol. 2024; 25(8): 1038-52.
- Bex A, van Thienen JV, Schrier M, et al. A Phase II, single-arm trial of neoadjuvant axitinib plus avelumab in patients with localized renal cell carcinoma who are at high risk of relapse after nephrectomy (NEOAVAX). Future Oncol. 2019; 15(19): 2203-9.
- Burgers FH, Graafland NM, Lagerveld BW, et al. 1481TiP A prospective, randomized phase II trial of neoadjuvant immunotherapy in primary clear cell renal cancer at risk for recurrence or distant metastases: The NESCIO trial. Annal Oncol. 2022; 33(7): S1224.
- Ursprung S, Mossop H, Gallagher FA, et al. The WIRE study a phase II, multi-arm, multi-centre, non-randomised window-of-opportunity clinical trial platform using a Bayesian adaptive design for proof-of-mechanism of novel treatment strategies in operable renal cell cancer - a study protocol. BMC Cancer. 2021; 21(1): 1238.