(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the session Progress and Controversies in oncological urology from the EAU Section of Oncological Urology. Dr. Viktor Grünwald debated the switch to second-line systemic treatment in oligoprogression after first-line systemic therapy in RCC.
Dr. Grünwald highlighted the available treatment options for oligoprogression after first-line systemic therapy in renal cell carcinoma (RCC). One key decision is whether to pursue single-modality or multimodality treatment, a choice often made in multidisciplinary conferences. Available options include surgery, radiotherapy, and switching to second-line systemic therapy as illustrated below.

The European Association of Urology (EAU) and European Society for Medical Oncology (ESMO) guidelines recommend switching to a vascular endothelial growth factor receptor (VEGFR) inhibitor that has not been previously administered. Available options include:
- Cabozantinib
- Axitinib
- Lenvatinib-everolimus
- Pazopanib
- Sunitinib
- Tivozanib
- Belzutifan®

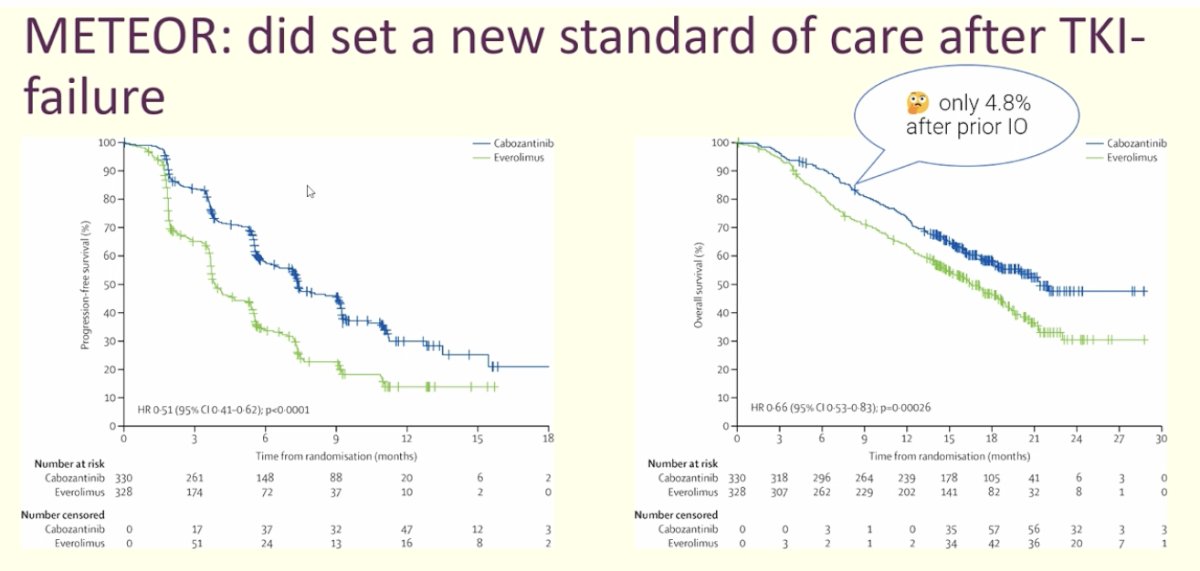
We strongly recommend cabozantinib based on data from the METEOR trial, which demonstrated a significant improvement in OS and PFS, establishing cabozantinib as the standard of care after TKI failure. However, a key limitation is that the study did not include patients who received first-line immunotherapy—only 4.8% had prior immunotherapy, which is now the standard in this setting. As a result, the applicability of these findings to the current treatment landscape remains uncertain.1
Several trials have evaluated cabozantinib in the setting of contemporary first-line therapies. The CANTATA study assessed telaglenastat—an agent targeting tumor microenvironment metabolism—plus cabozantinib versus placebo plus cabozantinib. Notably, 62% of patients had received prior immunotherapy. Unfortunately, the combination failed to show benefit.3
Another key study, CABOPOINT, led by Dr. Albiges, specifically evaluated cabozantinib in a modern cohort where 100% of patients had received prior immunotherapy. Taken together, multiple phase 3 studies provide strong evidence suggesting that cabozantinib remains a leading option for second-line therapy after progression.

Moreover, the combination of lenvatinib and everolimus is another option for previously treated patients. This regimen has been shown to significantly improve PFS following TKI therapy. Additionally, a separate study, in which 26% of patients had received prior immunotherapy, aimed to determine the optimal dosing of lenvatinib plus everolimus in this setting and showed a signal towards improved PFS in patients treated with the Lenvatinib 18mg + everolimus.4

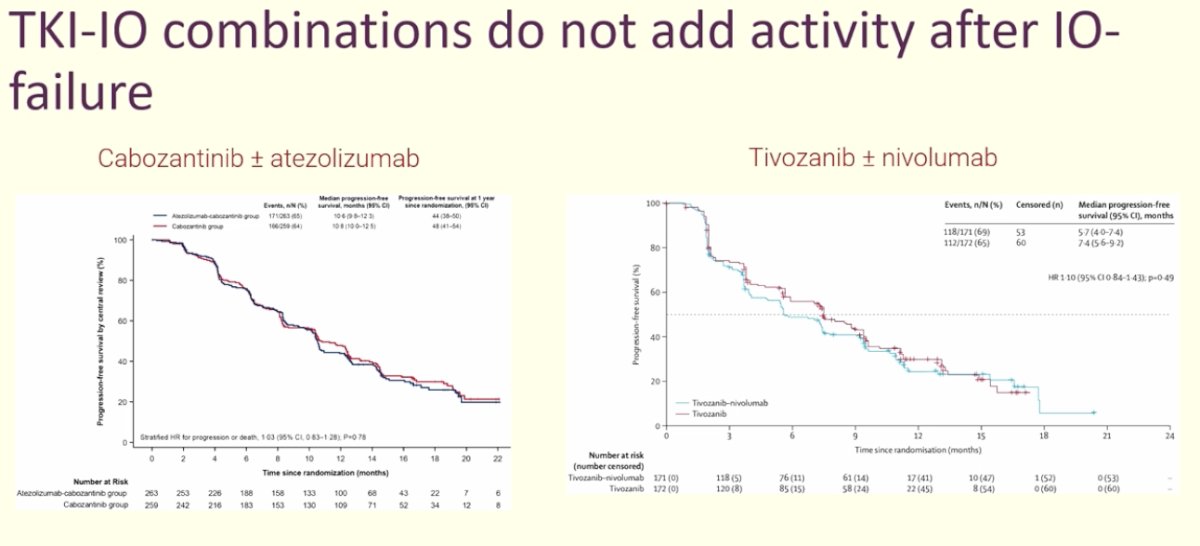
Dr. Grünwald highlighted that medical oncologists often combine treatments to enhance therapeutic activity. However, he presented data on two TKI-IO combinations that failed to show an additive effect after IO failure: cabozantinib with or without atezolizumab in the CONTACT-03 trial5 and tivozanib with or without nivolumab in the TiNivo-2 study.6 As shown in the curves below, there was no significant difference in PFS between the combination therapy and TKI monotherapy.
Dr. Grünwald concluded his presentation with the following key messages:
- Post-progression therapy should be an individualized decision, typically made within a multidisciplinary team.
- TKI therapy remains a life-prolonging option after first-line failure, a principle reinforced over the past decade.
- Importantly, TKI-IO combinations should not be used in later lines of therapy, as they have not demonstrated added benefit.
Presented by: Viktor Grünwald, MD, PhD, Professor, Interdisciplinary Genitourinary Oncology, University Hospital Essen, Essen, Germany
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- Choueiri TK, Escudier B, Powles T, Tannir NM, Mainwaring PN, Rini BI, Hammers HJ, Donskov F, Roth BJ, Peltola K, Lee JL, Heng DYC, Schmidinger M, Agarwal N, Sternberg CN, McDermott DF, Aftab DT, Hessel C, Scheffold C, Schwab G, Hutson TE, Pal S, Motzer RJ; METEOR investigators. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016 Jul;17(7):917-927. doi: 10.1016/S1470-2045(16)30107-3. Epub 2016 Jun 5. PMID: 27279544.
- Tannir NM, Agarwal N, Porta C, Lawrence NJ, Motzer R, McGregor B, Lee RJ, Jain RK, Davis N, Appleman LJ, Goodman O Jr, Stadler WM, Gandhi S, Geynisman DM, Iacovelli R, Mellado B, Sepúlveda Sánchez JM, Figlin R, Powles T, Akella L, Orford K, Escudier B. Efficacy and Safety of Telaglenastat Plus Cabozantinib vs Placebo Plus Cabozantinib in Patients With Advanced Renal Cell Carcinoma: The CANTATA Randomized Clinical Trial. JAMA Oncol. 2022 Oct 1;8(10):1411-1418. doi: 10.1001/jamaoncol.2022.3511. PMID: 36048457; PMCID: PMC9437824.
- Motzer RJ, Hutson TE, Glen H, Michaelson MD, Molina A, Eisen T, Jassem J, Zolnierek J, Maroto JP, Mellado B, Melichar B, Tomasek J, Kremer A, Kim HJ, Wood K, Dutcus C, Larkin J. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015 Nov;16(15):1473-1482. doi: 10.1016/S1470-2045(15)00290-9. Epub 2015 Oct 22. Erratum in: Lancet Oncol. 2016 Jul;17(7):e270. doi: 10.1016/S1470-2045(16)30233-9. Erratum in: Lancet Oncol. 2018 Oct;19(10):e509. doi: 10.1016/S1470-2045(18)30672-7. PMID: 26482279.
- Pal SK, Puente J, Heng DYC, Glen H, Koralewski P, Stroyakovskiy D, Alekseev B, Parnis F, Castellano D, Ciuleanu T, Lee JL, Sunela K, O'Hara K, Binder TA, Peng L, Smith AD, Rha SY. Assessing the Safety and Efficacy of Two Starting Doses of Lenvatinib Plus Everolimus in Patients with Renal Cell Carcinoma: A Randomized Phase 2 Trial. Eur Urol. 2022 Sep;82(3):283-292. doi: 10.1016/j.eururo.2021.12.024. Epub 2022 Feb 21. PMID: 35210132.
- Pal SK, Albiges L, Tomczak P, Suárez C, Voss MH, de Velasco G, Chahoud J, Mochalova A, Procopio G, Mahammedi H, Zengerling F, Kim C, Osawa T, Angel M, Gupta S, Khan O, Bergthold G, Liu B, Kalaitzidou M, Huseni M, Scheffold C, Powles T, Choueiri TK. Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): a multicentre, randomised, open-label, phase 3 trial. Lancet. 2023 Jul 15;402(10397):185-195. doi: 10.1016/S0140-6736(23)00922-4. Epub 2023 Jun 5. PMID: 37290461; PMCID: PMC11017728.