(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to a thematic session on intravesical therapy for bladder cancer. Dr. Sima Porten discussed the emerging role of TAR as a novel intravesical drug delivery system.
What is the rationale for the development of an intravesical delivery system, such as TAR? The current treatment paradigm of both non-muscle and muscle invasive bladder cancer is highly toxic and morbid, stimulating the development of novel intravesical drug delivery systems with increased efficacy and decreased toxicity.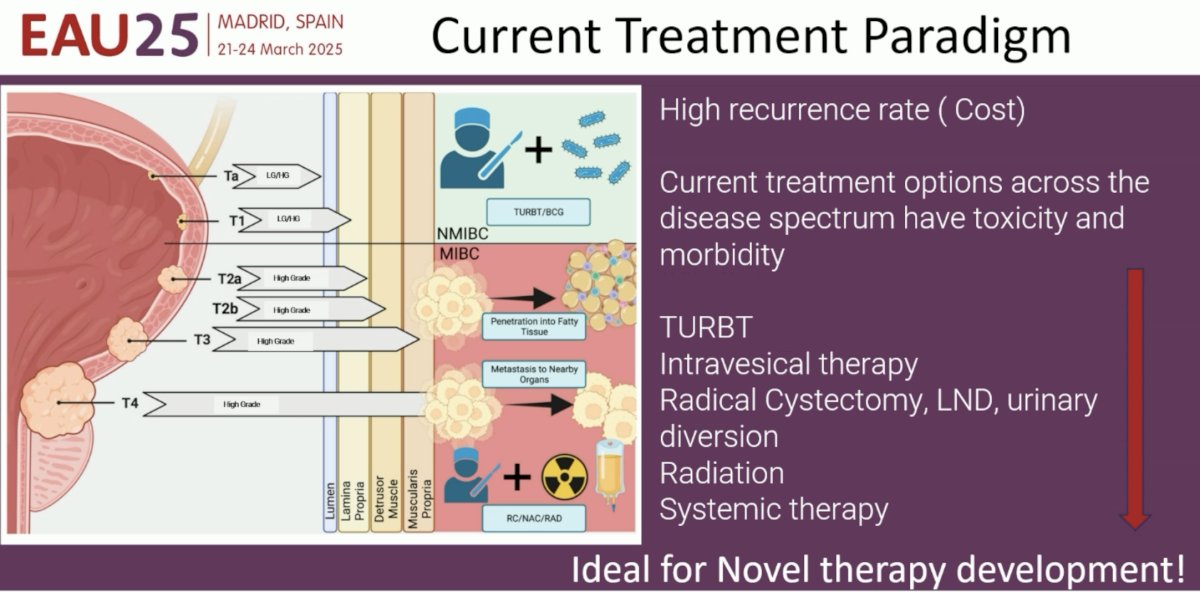
What are the limitations of classic drug delivery systems (i.e., intravesical instillations)? The contact time of intravesical drug instillations with the endothelium is typically only 1-2 hours, following which a patient voids, and has limited penetration. Furthermore, the drug concentration is diluted due to continuous urine production.
What are some potential solutions?
- Increase exposure via multiple treatments
- Develop a mode/device for sustained drug delivery
- Improve tissue penetration
Summarized below is the clinical development timeline of TAR, which Dr. Porten addressed step-by-step in her presentation: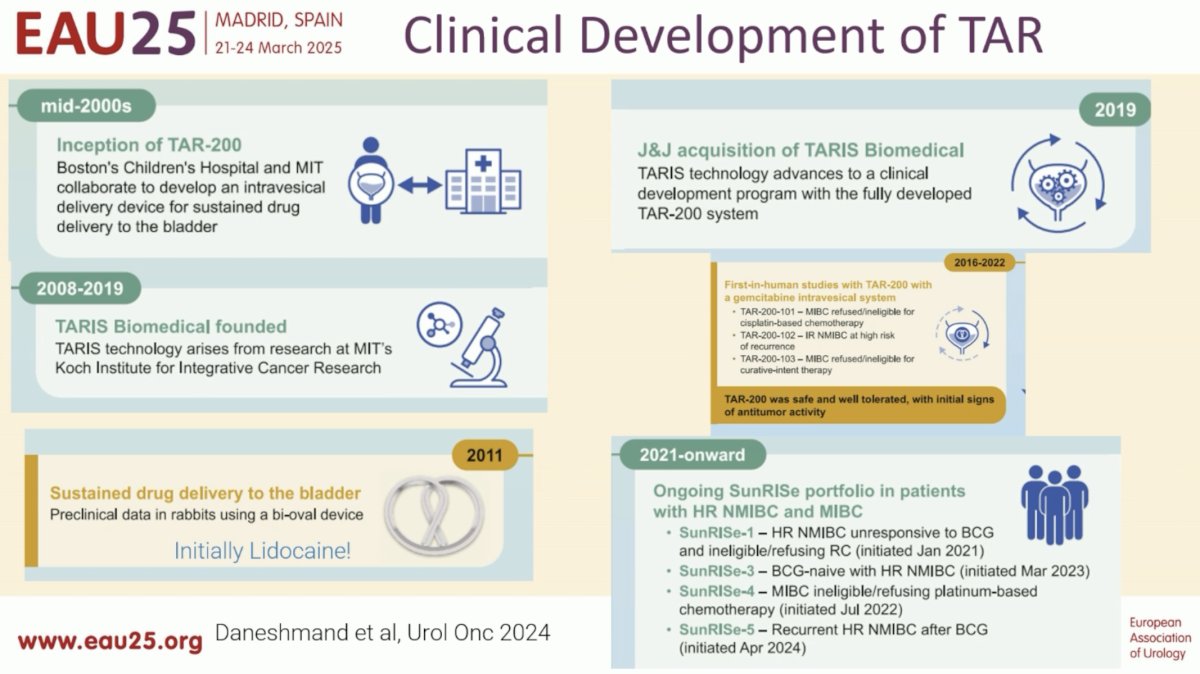
In the mid-2000s, Boston’s Children Hospital and MIT collaborated to develop an intravesical delivery device for sustained drug delivery to the bladder. This led to the inception of TAR.
What is the TAR device? It is a silicone dual lumen tube with a:
- Larger lumen: Solid drug core
- Smaller lumen: Flexible wire
It is freely mobile and compressible in the bladder. Importantly, the urea present in the urine allows for a functional osmotic drug pump using osmotic pressure for sustained diffusion.
Between 2008 and 2019, TARIS Biomedical was founded from research at MIT’s Koch Institute for Integrative Cancer Research. The TAR device containing lidocaine was initially tested in rabbits and was found to lead to effective analgesia and was safe.
Why was gemcitabine selected as the drug of choice for the TAR devices? Preclinical models demonstrated deep tissue penetration with gemcitabine. Gemcitabine is a prodrug that gets tri-phosphorylated intracellularly to dFdCTP. With prolonged intravesical exposure, this leads to increased intracellular doses. Additionally, gemcitabine may augment anti-tumor T-cell responses.
The TAR-200 device was instilled with gemcitabine (225 mg) and, as seen in the image below, led to a sustained release of gemcitabine intravesically over 7 days (blue curve), compared to intravesical gemcitabine instillations which were associated with a short-lived peak (green curve). Importantly, there were no detectable plasma levels of gemcitabine.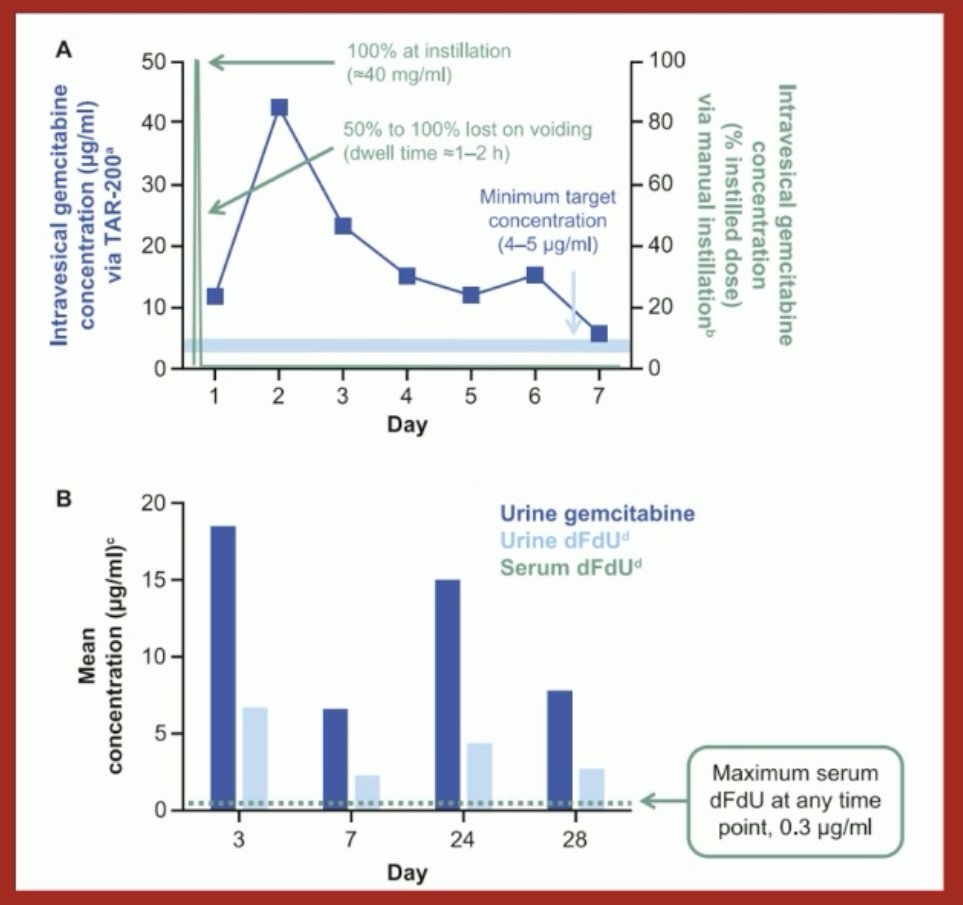
In 2019, J&J acquired TARIS Biomedical, and three first-in-human phase I studies evaluating TAR-200 were conducted between 2016 and 2022 (TAR-200-101, TAR-200-102, TAR-200-103). Overall, these trials demonstrated that TAR-200 was well-tolerated with only grade 1–2 adverse events (mainly urgency and frequency). There were no systemic signals/toxicity. Notably, 20–40% complete response rates were observed in these small cohorts.1
From 2021 onwards, four SunRISe trials have opened for recruitment: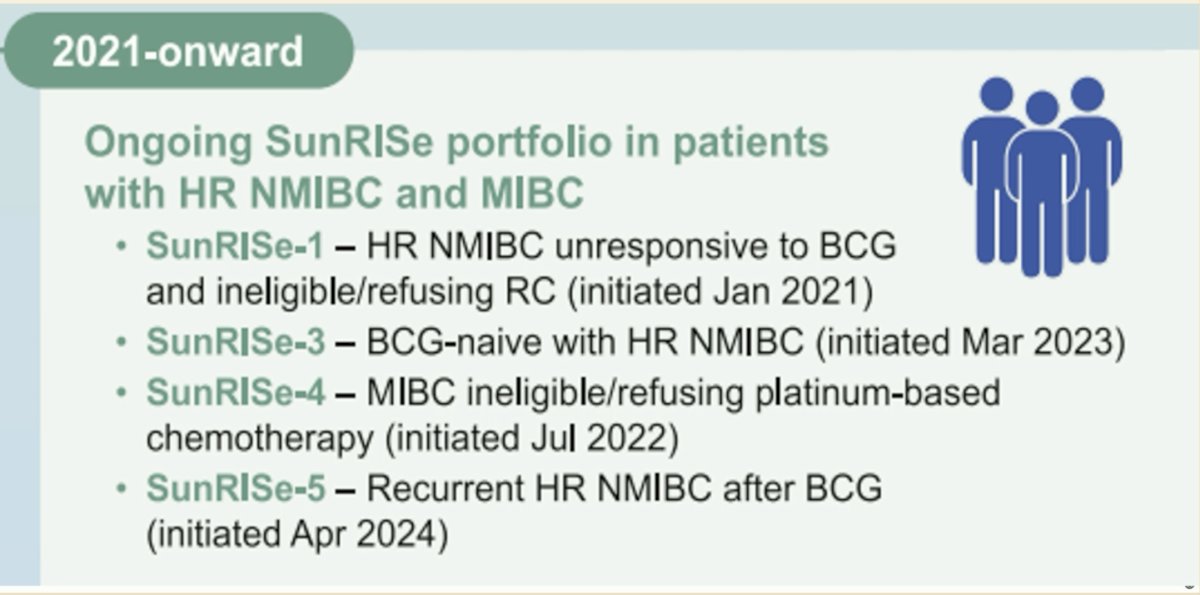
The SunRISe-1 phase IIb trial evaluated TAR-200 +/- cetrelimab (PD-1 inhibitor) in BCG-unresponsive high-risk NMIBC patients ineligible for or refusing radical cystectomy. This trial demonstrated that a complete response at any time was achieved in 83.5% of patients receiving TAR-200 monotherapy (n=85), with 82% of responders maintaining their response over a median follow-up of 9.2 months.
SunRISe-3 is a phase III trial of TAR-200 +/- cetrelimab versus BCG in BCG-naïve high-risk NIMBC patients. SunRISe-5 is a phase III trial of TAR-200 versus gemcitabine or mitomycin in patients with recurrent high-risk papillary NMIBC after BCG.
In contrast to SunRISe-1, 3, and 5, which were evaluated in the NMIBC setting, SunRISe-2 and 4 were performed for MIBC.
The SunRISe-2 trial was a phase III trial of TAR-200 + cetrelimab versus chemoradiotherapy in MIBC patients who either declined or were unfit for radical cystectomy. This trial was suspended early due to poor recruitment. However, Dr. Porten noted that results of this suspended trial are expected to be reported soon.
The SunRISe-4 trial evaluated TAR-200 +/- cetrelimab in the neoadjuvant setting prior to radical cystectomy in cisplatin-ineligible MIBC patients. As demonstrated in the trial schema below, eligible patients were randomized 5:3 to TAR-200 + cetrelimab (n=79) or cetrelimab monotherapy (n=41).
The combination of TAR-200 + cetrelimab was associated with a pathologic complete response of 42%, with a pathologic objective response of 60%. Conversely, in the cetrelimab only arm, the corresponding proportions were 23% and 36%, respectively.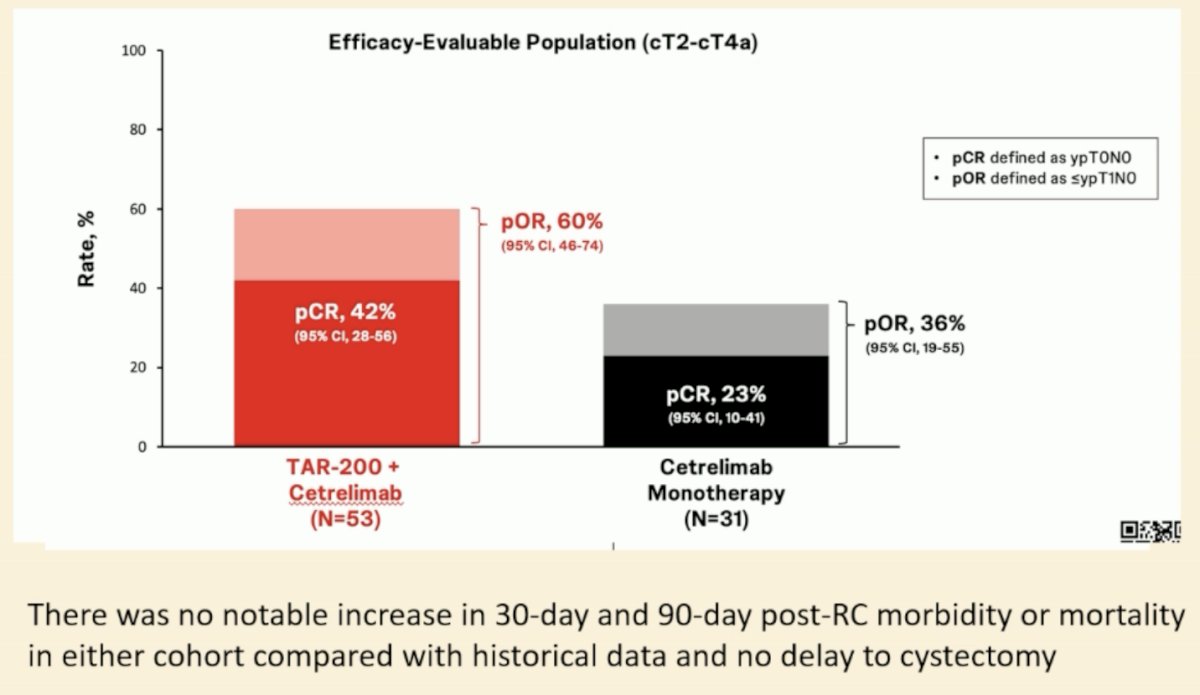
What are some future directions for TAR, given that this lumen can house other drugs? One potential candidate is erdafitinib. FGFR3 is highly mutated in NMIBC. Oral erdafitinib, a pan-FGFR inhibitor, is highly effective but has severe toxicity. This makes it challenging to prescribe for NMIBC patients. TAR-210, which houses erdafitinib, can be delivered into the bladder and has demonstrated:
- 90% RFS at 12 months in FGFR-altered high-risk NMIBC
- 86% complete response in intermediate-risk NMIBC
Dr. Porten concluded that the TAR system is an innovative answer to the large unmet need in patients with bladder cancer, and the future possibilities are endless.
Presented by: Sima Porten, MD, MPH, Associate Professor, Urologic Oncologist, Department of Urology, UCSF, San Francisco, CA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References: