(UroToday.com) Mr. Ryotaro Okazaki and colleagues from the University of Tsukuba and the National Institute of Advanced Industrial Science and Technology presented a breakthrough in artificial intelligence (AI) for bladder cancer detection. Despite the widespread use of white light cystoscopy, there remains a paucity in the ability of AI to detect flat lesions, small tumors, and carcinoma in situ (CIS), while also lacking practical processing speeds. Herein, Mr. Okazaki et al. aimed to develop a lightweight AI model optimized for real-time detection of difficult-to-detect lesions.
The team engineered a novel diagnostic framework that prioritized both detection precision and computational efficiency. Their model integrated elements of EfficientNetV2 and U-Net architectures, while also introducing an innovative "loss function fusion" strategy. A CNN architecture combining EfficientNetV2 and U-Net backbones was developed, and multiple loss functions, including Binary Cross-Entropy, Dice Loss, and Focal Loss, were incorporated to optimize learning for different lesion types. In addition to creating a standard baseline model trained with equal loss weighting, Mr. Okazaki's team generated specialized models focused on three distinct lesion characteristics, namely: the Challenging-Lesion Model, the Indistinct-Boundary Model, and the Small-Lesion Model. The outputs of these specialized models were then integrated into a final Fusion Model aimed at maximizing detection across lesion subtypes (Figure 1).

Figure 1: Diagnostic framework for detection.
Through extensive testing, they discovered that different weighting models excelled at detecting specific lesion features. By strategically fusing these models, they optimized performance for small, flat, and CIS lesions.
A robust dataset of 10,332 normal and 1,411 tumor images, including a high proportion (40.2%) of flat lesions, was meticulously labeled by urologists and pathologists based on shape, size, T stage, and malignancy grade, enabling a detailed lesion-specific analysis (Figure 2). Images were annotated by filling in lesion areas, and the dataset was split into 85% for training and 15% for testing. Data augmentation was applied to improve model robustness across variations in lesion appearance.
The fusion model delivered impressive detection improvements for the most elusive cases: detection rates for small tumors increased from 39.9% to 61.7%, flat lesion detection improved from 56.6% to 76.2%, and CIS lesion identification rose from 70.6% to 89.2%.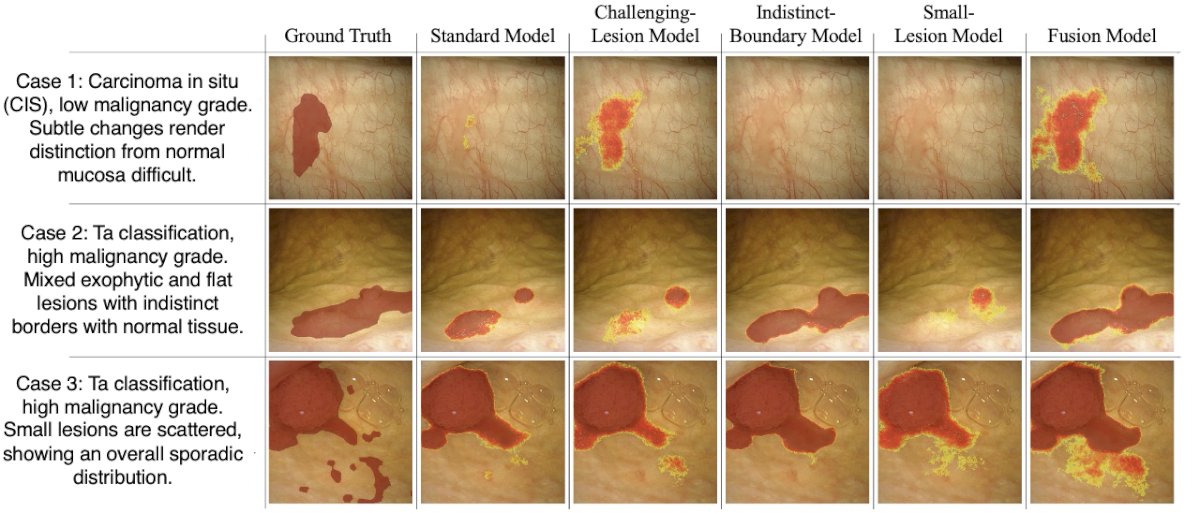
Figure 2: Comparison of specialized bladder lesion detection models across three clinical cases.
Overall model performance remained strong, achieving a sensitivity of 95.8%, a specificity of 98.8%, and a Dice coefficient of 0.822. Critically, this was accomplished using just 53 million parameters and at a processing speed of 14.9 frames per second on a standard laptop. These results demonstrate a viable AI model capable of real-time clinical application for challenging bladder cancer detection.
The presentation was concluded with the following remarks:
- Lightweight, high-precision AI model effectively overcomes two major barriers to AI deployment in bladder cancer care:
- Low detection rates for difficult-to-identify lesions.
- Prohibitive computational demands for real-time clinical use.
- This approach has the potential to significantly enhance early detection, lower recurrence rates, and improve patient outcomes, particularly by catching CIS lesions often missed by conventional cystoscopy.
Presented by: Ryotaro Okazaki, University of Tsukuba, Ibaraki, Japan
Written by: Mariah Hernandez, Research Specialist, Department of Urology, University of California, Irvine, @mariahch00 on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.