Dr. Su began by outlining the importance of surgical innovation and what has already been achieved within minimally invasive surgery. While most urologists in the 1990s were trained via laparoscopy. With the emersion of single-port robotic surgery, however, comes a steep learning curve and suspicion regarding its true benefit in comparison to widely adopted multiport robotic surgery systems across the globe.
Dr. Simone Crivellaro from the University of Illinois, Chicago, took the stage first in this crossfire to present his case on why SP robotic surgery is superior to current MP robotic surgery. First, Dr. Crivellaro outlined the most common misconceptions regarding single-port robotic surgery – that it is not “real innovation” and is considered a “gimmick”. He also highlighted that MP has reached its technological limit, and that SP is the only real innovation in robotic surgery since MP has only undergone iterations since its introduction in the 1990s.

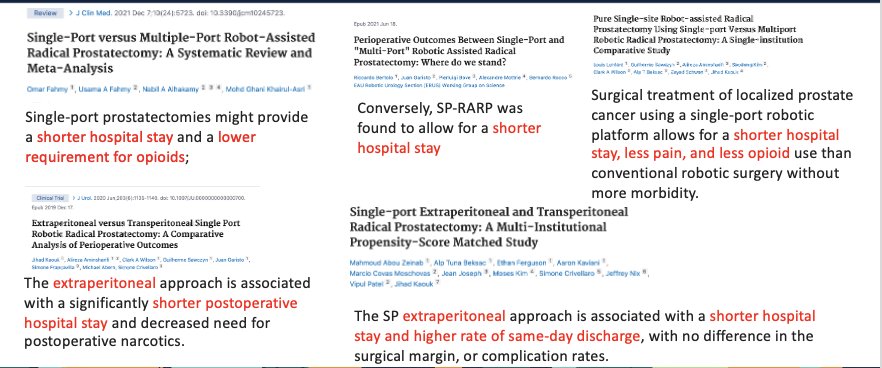
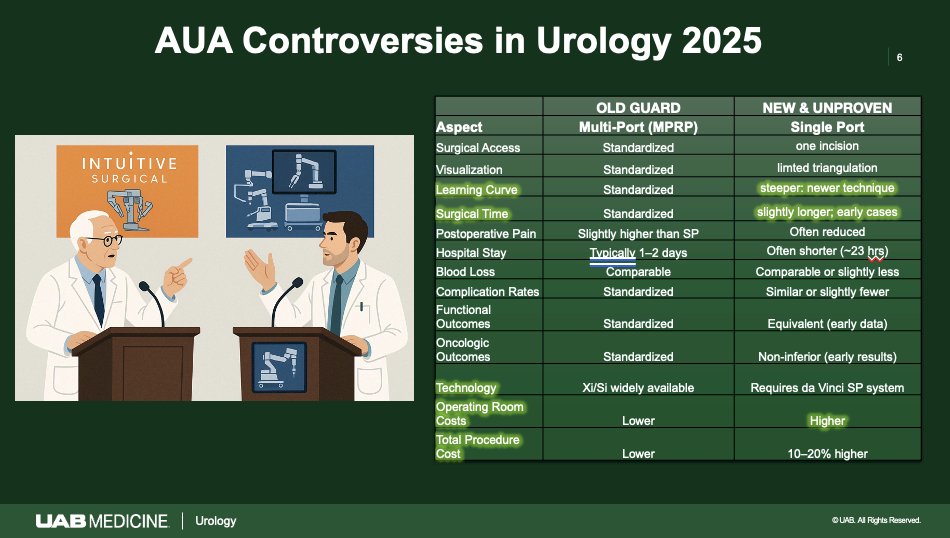
Dr. Crivellaro outlined how SP is the most minimally invasive form of surgery that has been achievable since the introduction of minimally invasive surgery, and while multiple surgeons complain of the steep learning curve, it is inevitable with technological advancement, and necessary. He stressed that while SP is innovative and MP is widely applied, neither is the only option, as “one size does not fit all,” and patients must be cared for case by case when accounting for what type of robot to use in their surgical interventions. Nonetheless, literature regarding SP has shown to significantly improve extraperitoneal approaches, which in turn allow for lower opioid requirements by patients due to lower pain reports, shorter postoperative hospital stays, and a higher rate of same-day discharge. potentially provide shorter hospital stay, lower requirements for opioids due to lower pain reports from patients, and allow for more extraperitoneal surgery.
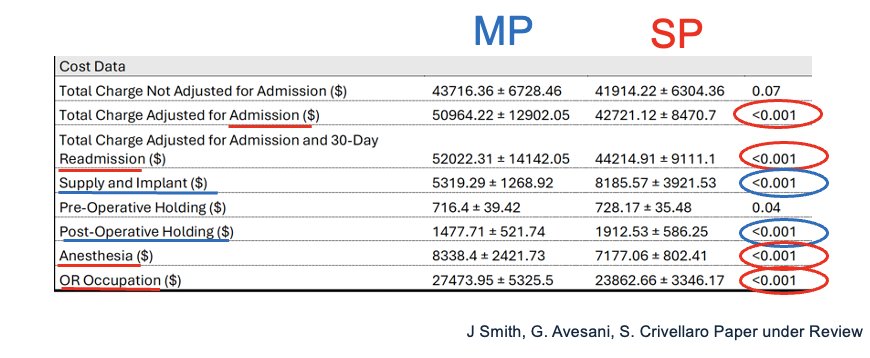
After highlighting what the literature says about SP robotic surgery, Dr. Crivellaro debunked the myth that SP was more expensive than MP through providing data from one of his studies - a comparative cost analysis of single-port and multi-port robotic assisted prostatectomy at a single institution highlighting that the total charge adjusted for admission, 30-day readmission, anesthesia, and OR occupation were all significantly less in SP as compared to MP. Moreover, supply and implant, and post-operative holding costs were also significantly less.
Where retroperitoneal approaches in minimally invasive surgery, such as SP or MP robotic surgery, allow for optimized postoperative recovery, SP allows for the application of this approach more often than MP does, thus reducing complications according to one of Dr. Crivellaro’s studies quoted in his argument for SP over MP. Moreover, there are decreased complications in obese or more complex patients, reducing the anesthesiologic impact of surgery on patients receiving SP as compared to MP robotic surgery.

Lastly, Dr. Crivellaro touched on the benefits of SP for surgeons, including increased versatility, increased efficiency, and the learning curve. For risk of post-operative complications to be reduced close to 0, simple prostatectomies required between 30-50 prior surgeries of surgeon experience, robot assisted laparoscopic radical prostatectomies required around 80 surgeries, and robot assisted partial nephrectomies required around 160 prior surgeries of experience.

Dr. David Lee from the University of California, Irvine, then took the stage to rebut Dr. Crivellaro’s points in support of SP. in support of MP over SP. Dr. Lee touched upon the track record of MP growth versus SP growth. Where procedures with MP have increased by 2.65 million cases between 2019 and 2024, SP cases have increased by only 3000 cases.

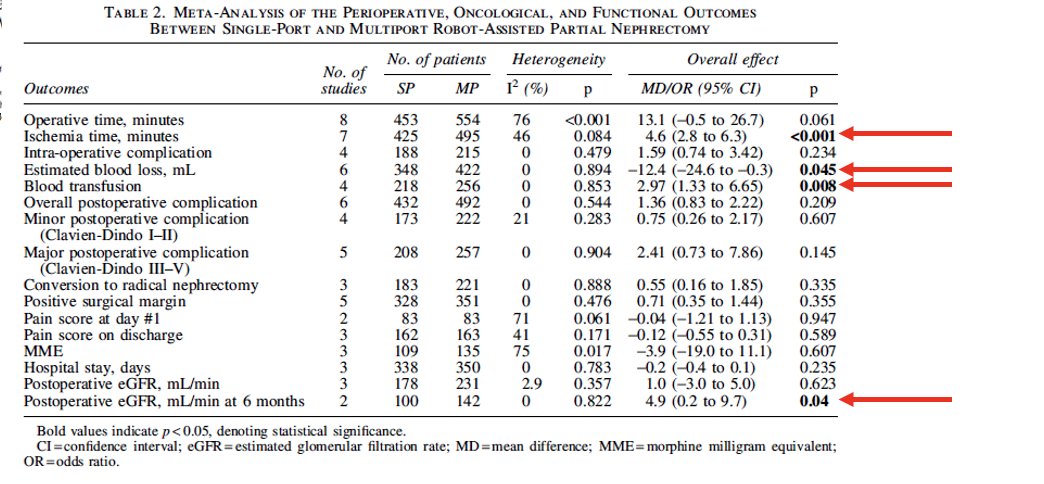
Moreover, Dr. Lee touched upon how certain perioperative parameters, including ischemia time, estimated blood loss, and rates of blood transfusion were all still higher among SP cases as compared to MP cases of robotic assisted partial nephrectomy. Postoperative eGFR in mL/min was also superior in MP cases as compared to SP cases within 6 months postoperatively.
Although these statistics are in favor of MP robotic surgery for partial nephrectomy, Dr. Lee also supported Dr. Crivellaro’s earlier point that SP robotic surgery resulted in lower pain scores, hospital stay in days, urinary catheterization time, and console time. Moreover, SP was significantly more expensive than MP ($3,544.18 versus $1,471.09 when comparing all components of the robotic system set-up).

Dr. Lee touched back on Dr. Crivellaro’s data on learning curves during SP implementation, and highlighted how 160 procedures worth of surgical experience is still quite significant and not worth the weight of the learning curve that SP poses on trainees and surgeons alike, since there is still a greater risk of complications prior to that gained experience that could be otherwise avoided if MP robotic surgery was done instead. While the familiarity and extensive hands-on experience of MP robotic surgery provides surgeons comfort, SP offers a new, valuable, and exciting approach to minimally invasive surgery that is garnering a lot of attention from surgeons globally.
To speak in favor of SP, Dr. Jeffrey Nix, visiting from the University of Alabama, took the podium. Dr. Nix jumped right into his argument that “multiport was never the point anyway” in the pathway of innovation in minimally invasive surgery. The learning curve argument was also refuted through showing a clip of what surgeons were saying about the applications of robotic surgery in an era where laparoscopy was the standard. Similar arguments that arose around MP robotic surgery versus laparoscopy arise now when speaking about SP robotic surgery versus MP robotic surgery, and thus show an ongoing cycle in which audiences react similarly yet adopt these changes and technological advancements out of recognition of the significant value to our patients.
Dr. Nix stressed on the same point as Dr. Crivellaro earlier that the whole point of minimally invasive surgery was never to stop, but to constantly evolve towards even less invasive techniques with less impact on patients: “We did not stop at hand-assisted laparoscopic surgery, so why in the world would we stop at multi-incision robotics when we can continue to evolve? The entire journey through SSILS was a recognition of this.”
Next, Dr. Nix spoke about the importance of different patient scenarios in the selection of SP robotic surgery. For patients requiring peritoneal dialysis who had never needed hemodialysis, SP allows for extraperitoneal approaches effectively, which allows a complex patient to go home the same day. Moreover, patients with prior total colectomies with ileo-anal pouches who would otherwise have been very complex in a MP robotic surgery approach were able to go home the same day after a SP transvesical prostatectomy. SP transvesical bladder neck reconstruction in a patient after anastomosis failure from a RARP was also possible, which would not have been as easily achievable with MP robotic surgery.
Dr. Nix touched on the popular argument of the extensive learning curve required to learn SP as compared to MP robotic surgery. MP remains low outside of the peritoneum due to difficulty in access, whereas SP has made these approaches easier through lower anterior access, allowing for safer diversification in robotic procedures. Literature showed that the majority of US residents did not see SP as negatively affecting their training. Despite over 70% of programs not having a dedicated SP didactics set up & 65% felt their programs favored MP over SP, only 26% of respondents felt that he learning curve for SP was too steep.
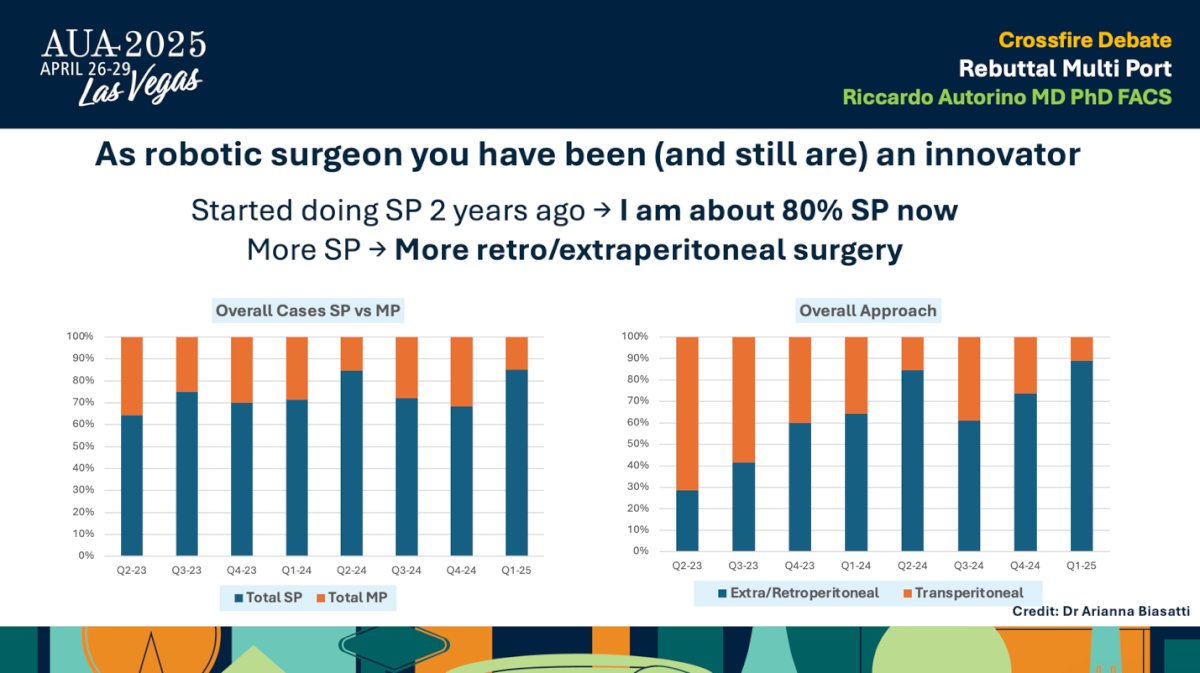
Finally, we were joined by Dr. Riccardo Autorino from the Rush University Medical Center in Chicago, who came with a rebuttal for MP robotic surgery. Where previous speakers focused on SP versus MP, Dr. Autorino focused on how crucial it was to take a look at patients case by case and recognize that one size does not in fact fit all. Many recognize that current surgeons are all MP trained and thus feel more familiar and comfortable implementing it in their own practice. Dr. Autorino himself touched upon the evolution of his robotic surgical practice, where 80% of his current cases are now SP and thus done retro or extraperitoneally.
Dr. Autorino challenged the binary vision that a large number of current surgeons possess, where it must be one or the other. Adopting SP does not mean abandoning MP altogether. Rather than pitting the two technological advancements against each other, Dr. Autorino challenges the audience to consider putting them together instead to create “tailored robotic surgery.”
There are expanding indications for certain MP robotic surgeries in the upper urinary tract, which still call for the use of MP. However, it is important to realize that not all procedures are effectively done through MP, and picking the correct surgical modality is the most crucial aspect.


Dr. Autorino touches on this point further by providing examples of partial nephrectomy cases that would either require MP or SP:


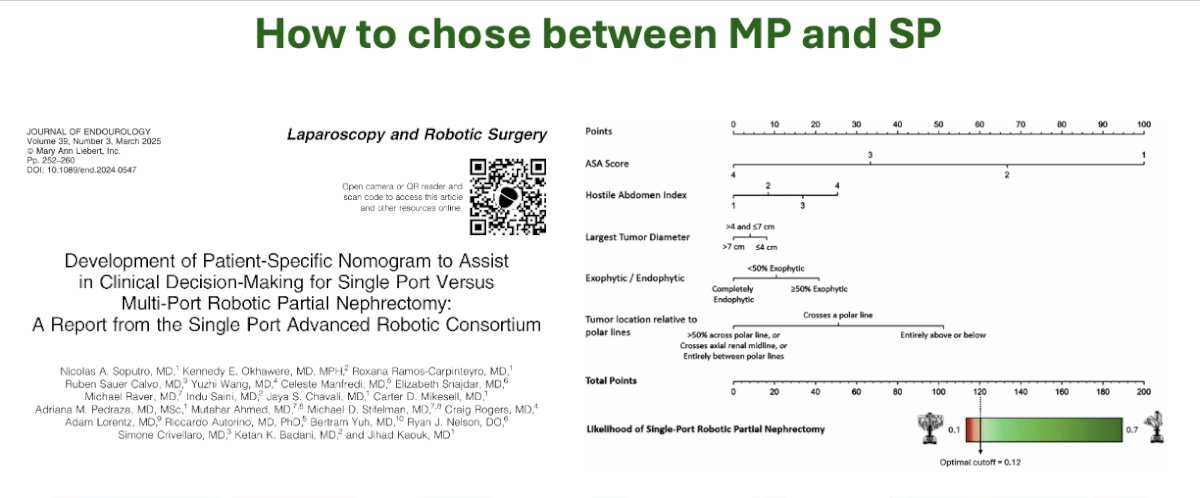
The decision regarding opting for MP versus SP should be made with consideration of multiple aspects and characteristics of the patients’ health and disease. Dr. Autorino references a study on the development of patient specific nomograms to assist in clinical decision-making for single port versus multi-port robotic partial nephrectomy. Utilization of tools like this allows for expansion of surgical skillset instead of having to entirely shift from one type of practice to another.
Although anything can be done with SP, that does not mean it should be, as what needs to be done is what is ultimately best for the patient. MP will still be the better option in multiple procedures, and may still be the safer option in specific surgeries.
To wrap up the crossfire debate on SP versus MP, Dr. Su asked the audience through a brief survey if they would opt for either only MP or SP. Over 70% of the audience opted for MP. When asked what they would choose if they had both choices prior to a surgery, 68% of the audience said it depends on the procedure, 28% would choose MP, and 4% said they would opt for SP.
While technological advancements in minimally invasive surgery may be pointing towards SP, speakers agree that more experience and resident training with SP, alongside more literature, are required to make a concrete statement on the progression of robotic surgery going forward.
Moderated by: Li-Ming Su, Chairman of Urology, University of FloridaExpert Panel:
- Simone Crivellaro, Vice Chair, Lawrence Ross Endowed Professor of Urology, Director of Minimally Invasive Urology, University of Illinois College of Medicine, Chicago, IL, USA
- David Lee, Professor and Executive Vice Chair of Urology, Director of the Robotic Urologic Surgery Fellowship, University of California, Irvine, CA, USA
- Jeffrey Nix, Joe A. Chambliss Endowed Professor of Urology, Director of Robotic Surgery, University of Alabama at Birmingham, AB, USA
- Riccardo Autorino, Professor of Urology, Director of Surgical Innovation and Clinical Research, Rush University Medical Center, Chicago, IL, USA