(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Elisabeth Heath discussing 177Lu-PSMA-617 in combination with androgen receptor pathway inhibitors versus 177Lu-PSMA-617 alone for the treatment of metastatic castration resistant prostate cancer (mCRPC). The 5-year relative survival rate for mCRPC is only approximately 25%. Based on the VISION trial,1 177Lu-PSMA-617 received initial US approval in 2022 for patients with PSMA-positive mCRPC previously treated with 1+ taxane and 1+ androgen receptor pathway inhibitor, with further US label expansion in 2025 based on the results of the PSMAfore trial2 to include patients treated with androgen receptor pathway inhibitor therapy for whom deferring taxane-based chemotherapy was appropriate. 177Lu-PSMA-617 is currently under investigation in combination with an androgen receptor pathway inhibitor in those with metastatic hormone-sensitive prostate cancer (PSMAddition trial: NCT04720157). This observational study was performed to assess the effectiveness of 177Lu-PSMA-617 in combination with an androgen receptor pathway inhibitor in patients with mCRPC in the real-world setting.
This was a retrospective cohort study of adults with mCRPC in the PRECISION data platform, a comprehensive database of prostate cancer patients compiled from diverse clinical settings in the US. Patients who received 177Lu-PSMA-617 during March 23, 2022 – June 27, 2025 were identified, among whom two cohorts were selected for inclusion: those who had evidence of androgen receptor pathway inhibitor use (apalutamide, darolutamide, abiraterone, or enzalutamide) at any time during 177Lu-PSMA-617 treatment (concomitant androgen receptor pathway inhibitor cohort), and those who had no other treatment for mCRPC during 177Lu-PSMA-617 treatment (no concomitant therapy cohort):
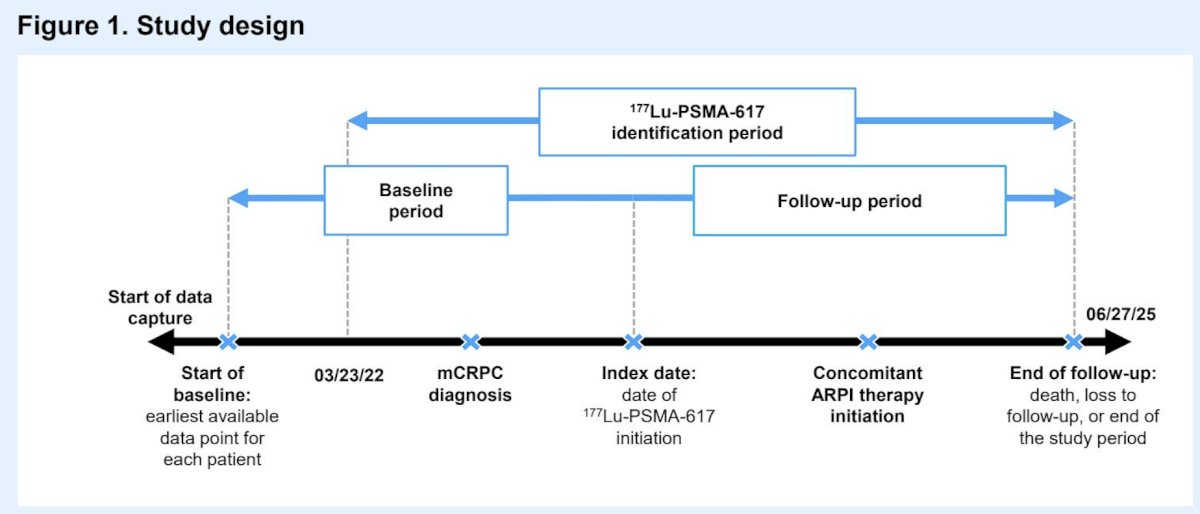
The index date was initiation of 177Lu-PSMA-617, and patient characteristics and PSA responses were evaluated descriptively. Progression free survival, defined as the time from 177Lu-PSMA-617 initiation to disease progression or death, was estimated using Kaplan–Meier analysis.
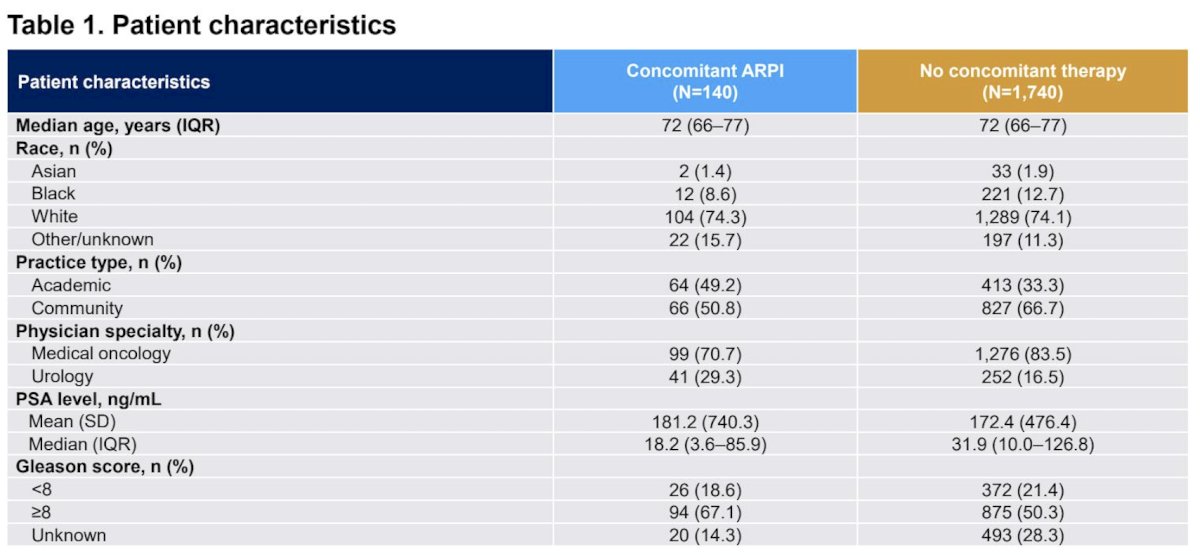
A total of 1,880 patients treated with 177Lu-PSMA-617 were identified, 140 in the concomitant androgen receptor pathway inhibitor cohort and 1,740 in the no concomitant therapy cohort. The median age was 72 years, and demographic characteristics were balanced between the groups, except that median baseline PSA was lower in the concomitant androgen receptor pathway inhibitor cohort when compared with patients in the no concomitant therapy cohort (18.2 ng/mL versus 31.9 ng/mL):
Before 177Lu-PSMA-617 initiation, 94.3% and 73.6% of patients in the concomitant androgen receptor pathway inhibitor and 80.9% and 56.7% in the no concomitant therapy cohort had received ≥1 prior androgen receptor pathway inhibitor and ≥1 prior taxane, respectively. PSA response rates were broadly comparable between cohorts, with slightly higher rates observed among patients with no concomitant therapy:

The median progression free survival was 14.7 (95% CI 11.7–21.3) months among patients in the concomitant androgen receptor pathway inhibitor cohort versus 12.5 (95% CI 11.5–13.6) months in the no concomitant therapy cohort:

The median overall survival was 20 months among patients in the concomitant androgen receptor pathway inhibitor cohort versus 15.7 months in the no concomitant therapy cohort:

In the multivariable analysis, after adjusting for patient and treatment characteristics, concomitant androgen receptor pathway inhibitor use was associated with a significantly lower risk of mortality (HR 0.664, 95% CI, 0.512–0.861). Higher prior treatment utilization was associated with an increased risk of mortality, while longer time from prostate cancer diagnosis to ¹⁷⁷Lu-PSMA-617 initiation was associated with a lower risk after adjusting for prior treatment utilization (HR, 0.964; 95% CI, 0.951–0.978).
Dr. Heath concluded her presentation discussing 177Lu-PSMA-617 in combination with androgen receptor pathway inhibitors versus 177Lu-PSMA-617 alone for the treatment of mCRPC with the following take-home points:
- Patients receiving concomitant androgen receptor pathway inhibitor had a higher median number of ¹⁷⁷Lu-PSMA-617 cycles, and longer progression free survival and overall survival compared with patients receiving no concomitant therapy
- The multivariable analysis, adjusted for patient and treatment characteristics, confirmed that concomitant androgen receptor pathway inhibitor was associated with significantly longer overall survival
- Median progression free survival, both with or without androgen receptor pathway inhibitor, was similar to that seen in patients in the PSMAfore trial. However, it was longer in those with concomitant androgen receptor pathway inhibitor than without
- Prospective randomized controlled studies are needed to confirm that the combination of ¹⁷⁷Lu-PSMA-617 with androgen receptor pathway inhibitor improves survival outcomes compared with ¹⁷⁷Lu-PSMA-617 alone
Presented by: Elisabeth I. Heath, MD, Mayo Clinic, Rochester, MN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.