(UroToday.com) The 2026 ASCO GU Annual Symposium hosted a prostate cancer poster session. Dr. Micah Ostrowski presented an analysis of survival outcomes of metastatic castration-resistant prostate cancer patients receiving 177Lu-PSMA-617, stratified by prior taxane exposure.
Lutetium Lu 177 vipivotide tetraxetan (Lu) is a prostate-specific membrane antigen (PSMA)–targeting radioligand therapy approved for patients with PSMA-positive mCRPC previously treated with androgen receptor pathway inhibitors (ARPIs) and considered appropriate to delay taxane chemotherapy. With regulatory approval expanding into taxane-naïve populations, limited data exist to guide treatment sequencing among patients progressing after ARPI therapy. Accordingly, the investigators sought to compare survival outcomes among patients with mCRPC receiving Lu based on the timing of taxane exposure.
This was an IRB-approved retrospective study using the US-based Flatiron Health electronic health record–derived database. Eligible patients had mCRPC with prior ARPI exposure who initiated Lu between December 19, 2018, and June 23, 2025. Patients were categorized into three cohorts based on taxane exposure relative to Lu initiation:
• Taxane before Lu
• Taxane after Lu
• Never received taxane
The key study endpoints included real-world overall survival (rwOS) and real-world time to next therapy (rwTTNT), estimated using Kaplan–Meier methodology with 95% confidence intervals.
Of 27,979 patients with metastatic prostate cancer in the Flatiron Health Database, 1,044 patients received Lu. After applying eligibility criteria requiring prior ARPI exposure and evaluable rwOS or rwTTNT data, the final analytic cohort included 850 patients:
• Taxane before Lu: n=466 (54.8%)
• Taxane after Lu: n=35 (4.1%)
• Never received taxane: n=349 (41.1%)

Median age overall was 74 years (IQR 68–80). Age distribution included:
• <65 years: ~15%
• 65–75 years: ~36%
• ≥75 years: ~48%
Most patients were White (~65%), with smaller proportions Black (~11%), Hispanic (~4%), Asian (~1%), or other/unknown categories. Regional representation was broad across the US geographic regions. Socioeconomic stratification by SES quintiles showed balanced representation, with slightly higher proportions in lower quintiles.

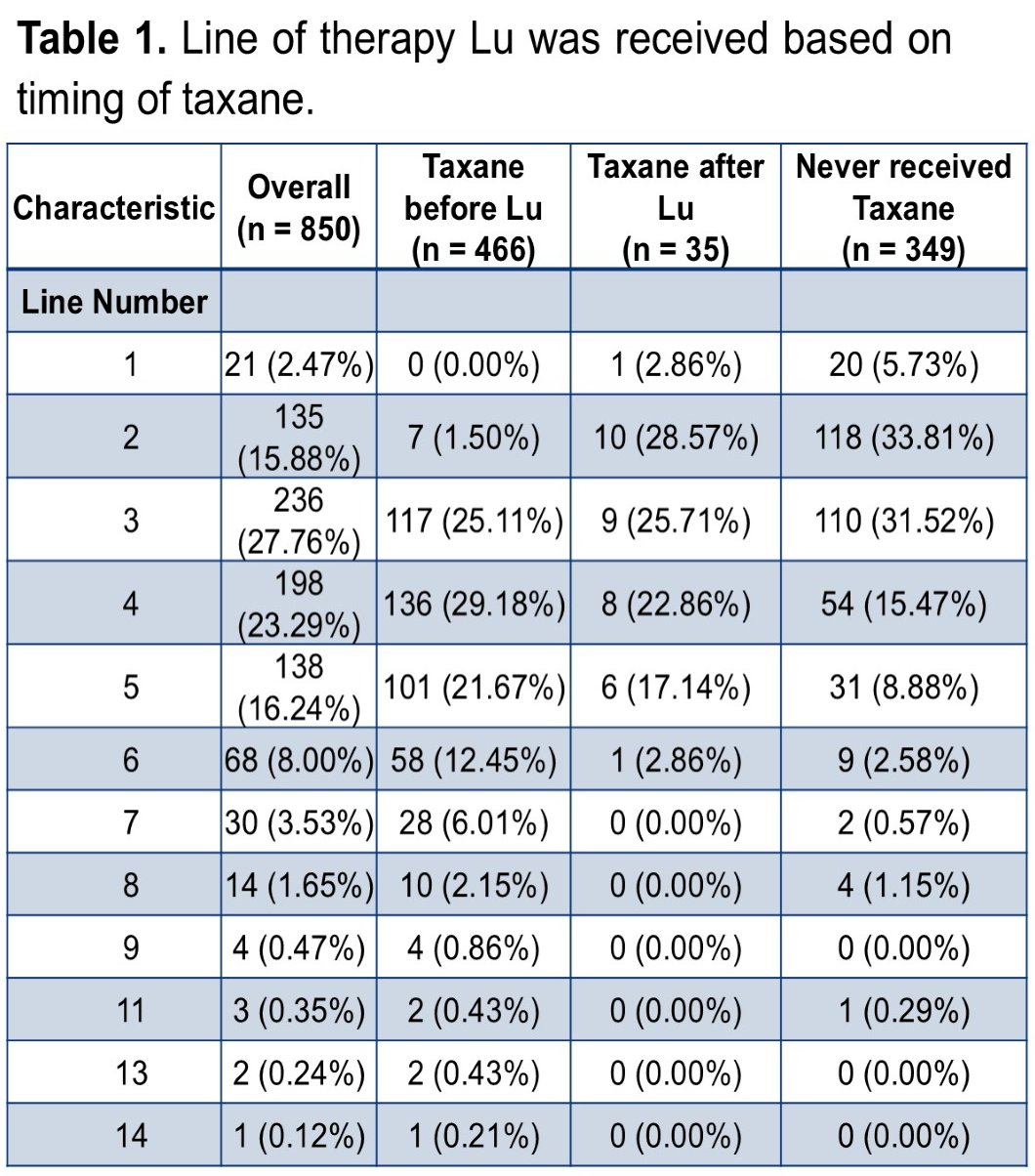
Timing of Lu relative to therapy line varied:
• First-line Lu use occurred primarily among taxane-naïve patients (~50%)
• Later-line use was more common among those with prior taxane exposure
Kaplan–Meier analyses demonstrated numerical differences in outcomes by taxane timing:
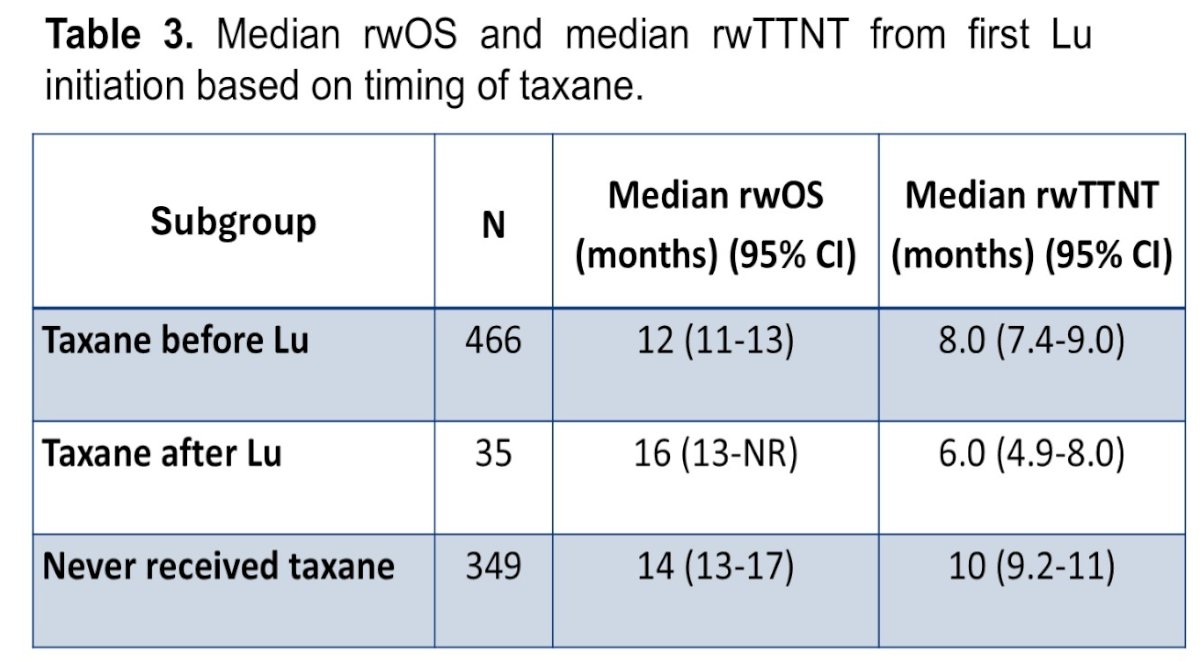
Real-world time to next therapy (rwTTNT):
• Taxane before Lu: 8.0 months (95% CI 7.4–9.0)
• Taxane after Lu: 6.0 months (95% CI 4.9–8.0)
• Never taxane: 10 months (95% CI 9.2–11)

Real-world overall survival (rwOS):
• Taxane before Lu: 12 months (95% CI 11–13)
• Taxane after Lu: 16 months (95% CI not reached)
• Never received taxane: 14 months (95% CI 13–17)
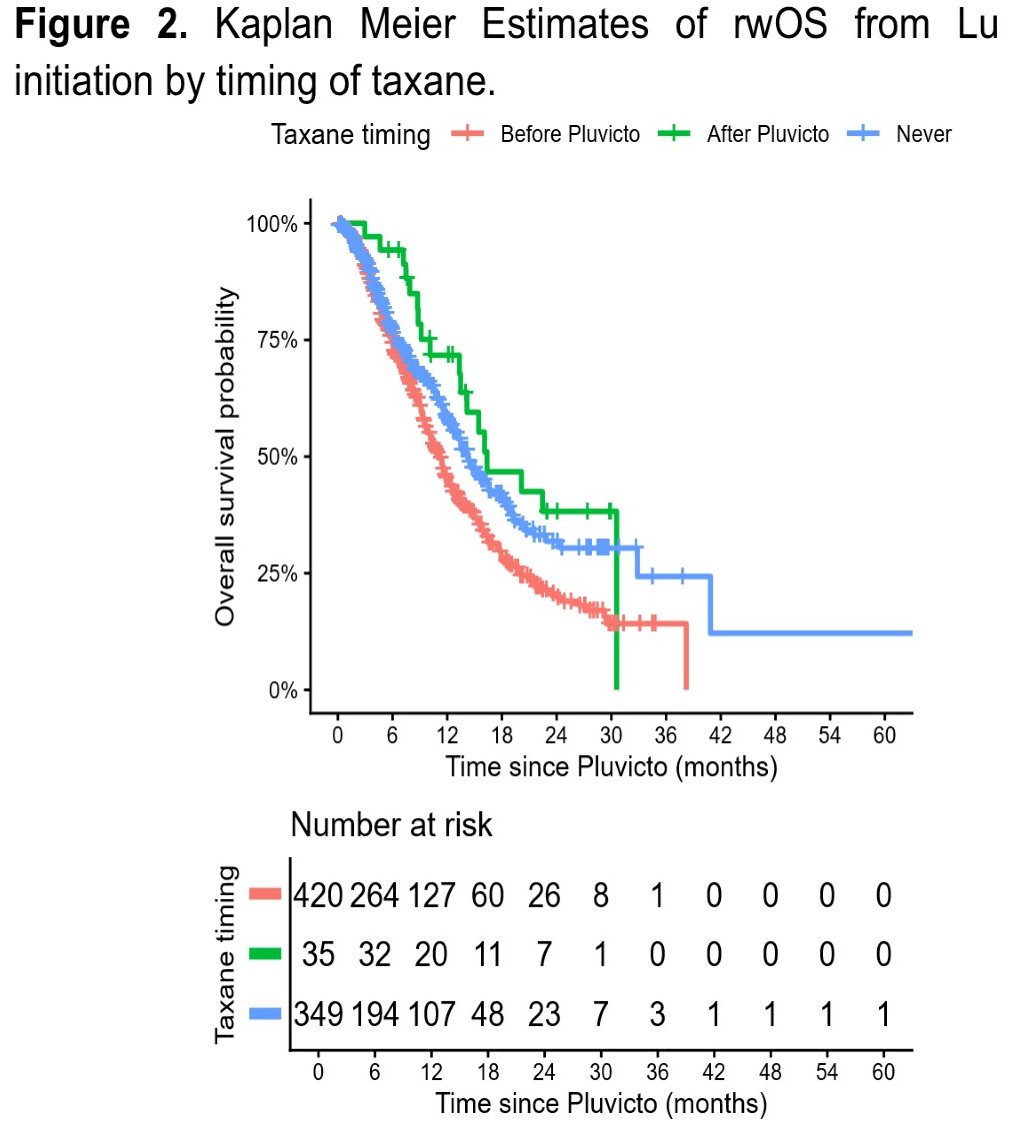
Graphical survival curves suggested slightly longer rwOS among patients receiving taxane after Lu and somewhat longer rwTTNT among taxane-naïve patients; however, interpretation is limited by cohort heterogeneity and smaller sample sizes in certain subgroups, particularly the post-Lu taxane cohort.
These data suggest:
• Lu demonstrates clinical activity regardless of prior taxane exposure
• Patients without prior taxane exposure may experience a longer time to subsequent therapy
• Differences in outcomes likely reflect patient selection, disease burden, and sequencing factors rather than intrinsic therapy efficacy differences.
Key study limitations were as follows:
• Retrospective observational design
• Potential confounding from treatment selection bias
• Missing data for certain endpoints
• Small sample size in the taxane-after-Lu subgroup.
Dr. Ostrowski concluded as follows:
- Numerical differences in rwTTNT and rwOS were observed with Lu based on the timing of taxane treatment. This may represent underlying patient and disease heterogeneity along with tumor evolution.
- Regardless of prior taxane exposure or not, Lu maintained effectiveness in patients with mCRPC.
- These results provide real-world data for patient counseling in the clinic and emphasize the need for randomized clinical trials in this setting for optimal treatment sequencing.
Presented by: Micah Ostrowski, MD, Resident Physician, Department of Internal Medicine, University of Utah, Salt Lake City, UT, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th–28th, 2026