(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Stephen Freedland discussing a post hoc analysis of EMBARK assessing secondary outcomes by prior definitive treatment in patients with high-risk biochemically recurrent prostate cancer treated with enzalutamide monotherapy. The phase 3 EMBARK trial demonstrated clinically meaningful improvement in metastasis-free survival and secondary efficacy endpoints with enzalutamide monotherapy versus leuprolide alone.1
Previously, metastasis free survival improvements with enzalutamide monotherapy versus leuprolide alone were observed in the subgroup of patients who had prior radiotherapy. At the GU ASCO 2025 annual meeting, Dr. Freedland and colleagues descriptively reported secondary endpoints for enzalutamide monotherapy versus leuprolide alone across prior definitive treatment subgroups.
Eligible patients had high-risk biochemically recurrent prostate cancer, with a PSA doubling time ≤9 months. Patients were randomized 1:1:1 to enzalutamide + leuprolide, leuprolide alone, or enzalutamide monotherapy. Secondary endpoints included time to PSA progression, first use of new antineoplastic treatment, distant metastasis, resumption of any hormonal therapy after treatment suspension, and symptomatic progression. Post hoc subgroup analyses descriptively compared secondary endpoints for enzalutamide monotherapy versus leuprolide alone in patients with radical prostatectomy only, radiotherapy only, or radical prostatectomy + radiotherapy.
In both treatment groups (enzalutamide monotherapy and leuprolide alone), most patients had prior had prior radical prostatectomy + radiotherapy. Regardless of prior definitive treatment, enzalutamide monotherapy versus leuprolide alone prolonged the key secondary endpoints of time to PSA progression (Pinteraction = 0.07):

Additionally, regardless of prior definitive treatment, enzalutamide monotherapy versus leuprolide alone prolonged the key secondary endpoints of time to use of new antineoplastic treatment (Pinteraction = 0.13):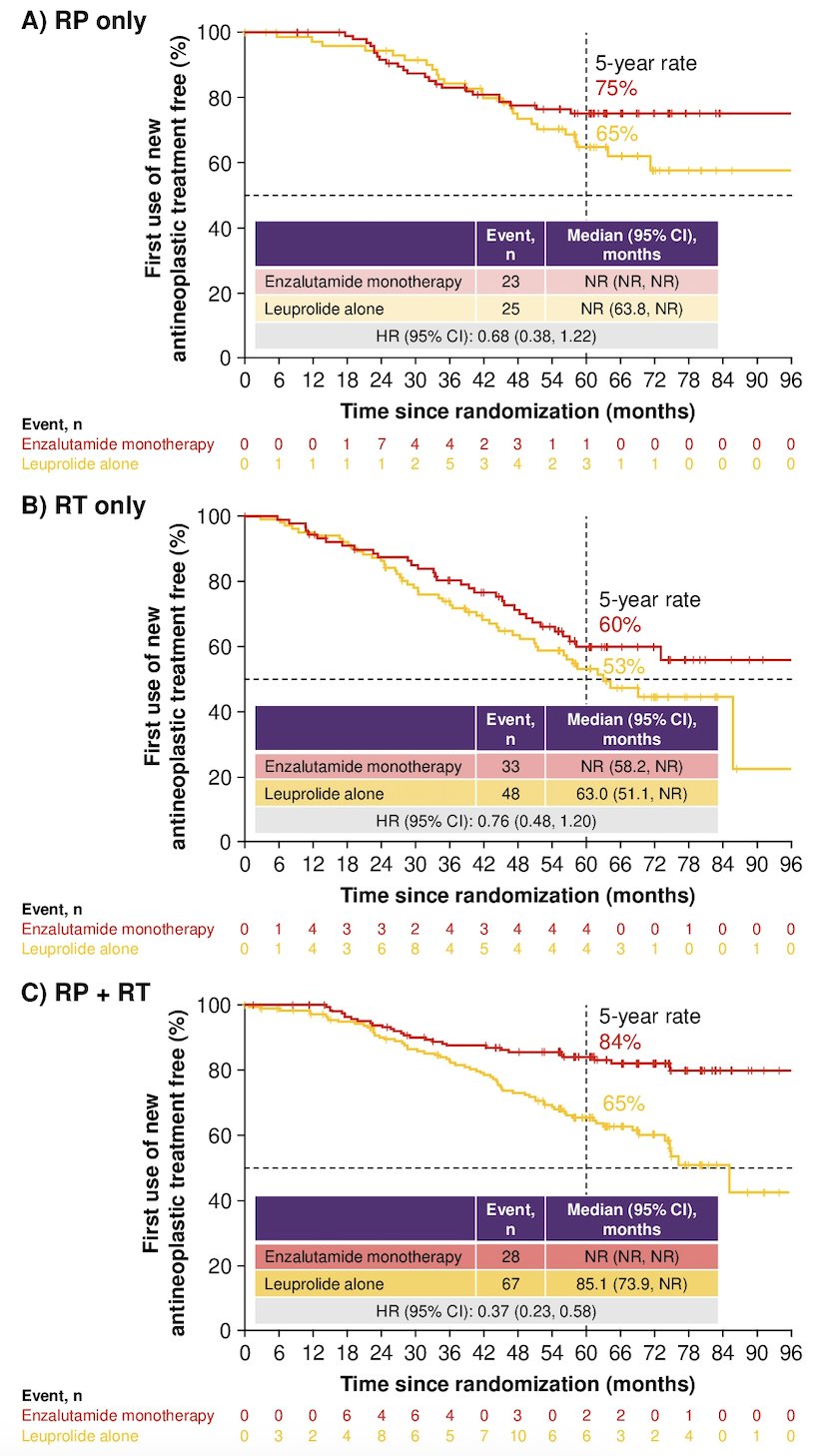
Similarly, improvements for enzalutamide monotherapy versus leuprolide for other secondary endpoints were independent of prior definitive treatment for time to distant metastasis (Pinteraction = 0.65) and symptomatic progression (Pinteraction = 0.59). Time to resumption of any hormonal therapy after treatment suspension favored leuprolide alone versus enzalutamide monotherapy independent of prior definitive treatment (Pinteraction = 0.18):
Dr. Freedland concluded his presentation discussing a post hoc analysis of EMBARK assessing secondary outcomes by prior definitive treatment in patients with high-risk biochemically recurrent prostate cancer treated with enzalutamide monotherapy with the following take-home points:
- Independent of prior definitive treatment, enzalutamide monotherapy versus leuprolide alone improved the time to PSA progression, first use of new antineoplastic treatment, distant metastasis, and symptomatic progression
- Time to resumption of any hormonal therapy after treatment suspension favored leuprolide alone versus enzalutamide monotherapy, independent of prior definitive treatment
- These results support the clinical benefits of enzalutamide monotherapy for patients with high risk biochemical recurrence regardless of prior definitive treatment. However, the small sample sizes of the nonrandomized subgroups and low event numbers should be considered when interpreting the results
Presented by: Stephen J. Freedland, MD, Department of Urology, Samuel Oschin Comprehensive Cancer Institute, Cedars-Sinai Medical Center, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: EMBARK Trial Subanalysis for High-Risk Biochemical Recurrent Prostate Cancer - Stephen Freedland
Reference: