(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Genitourinary (GU) Annual Symposium held in San Francisco, CA between February 13–15, 2025 was host to a rapid oral abstract prostate cancer session. Dr. Nicholas James presented the results of a STAMPEDE trial platform study evaluating the efficacy and safety of combining transdermal estradiol patches, as androgen deprivation therapy (ADT), with androgen receptor pathway inhibitors in metastatic (M1) prostate cancer.
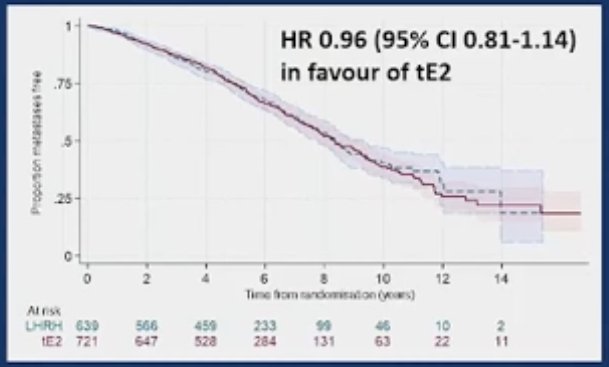
Recent phase III data (n=1360) has shown that starting ADT with transdermal estradiol patches is non-inferior in terms of metastasis-free survival (with similar overall survival) to luteinising hormone releasing hormone analogues (LHRHa) for locally advanced (M0) prostate cancer. For both M0 and M1 patients, transdermal estradiol has advantages in terms of:
- Improved quality of life
- Higher bone mineral density
- Less fatigue
- Less hot flushes
- Lower impact on sexual function
- Decreased hypertension, hyperlipidemia, and hyperglycemia side effect
- In contrast to oral estrogen, transdermal patches are not associated with an increase in the incidence of thromboembolic event.
However, there is currently no data on the use of androgen receptor pathway inhibitors (ARPIs) (abiraterone, enzalutamide, or apalutamide) with transdermal estradiol.
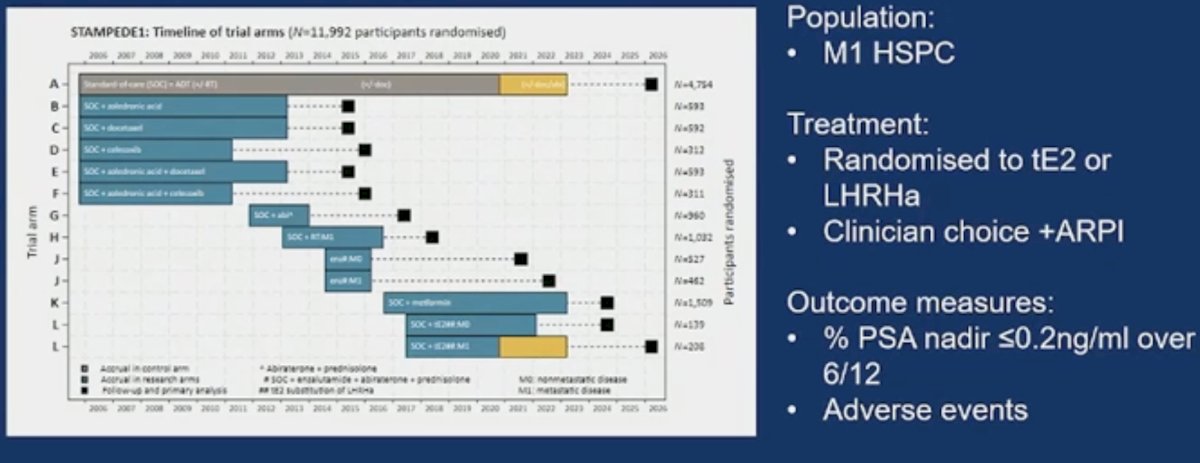
STAMPEDE [NCT00268476] is a multi-arm, multi-stage platform trial. This embedded phase II randomised study assessed the efficacy and toxicity in participants randomly allocated (1:1) to transdermal estradiol patches (releasing 100 mcg/24 hrs, 3 patches changed twice weekly once testosterone ≤1.7ng/ml) or LHRHa (standard doses) and scheduled to receive ARPIs (clinician’s choice).
The primary outcome measure was the proportion of patients achieving a PSA nadir of ≤0.2 ng/ml during the first 6 months. Secondary outcomes included:
- Other PSA parameters
- Testosterone ≤1.7 ng/ml at 12 weeks with transdermal estradiol
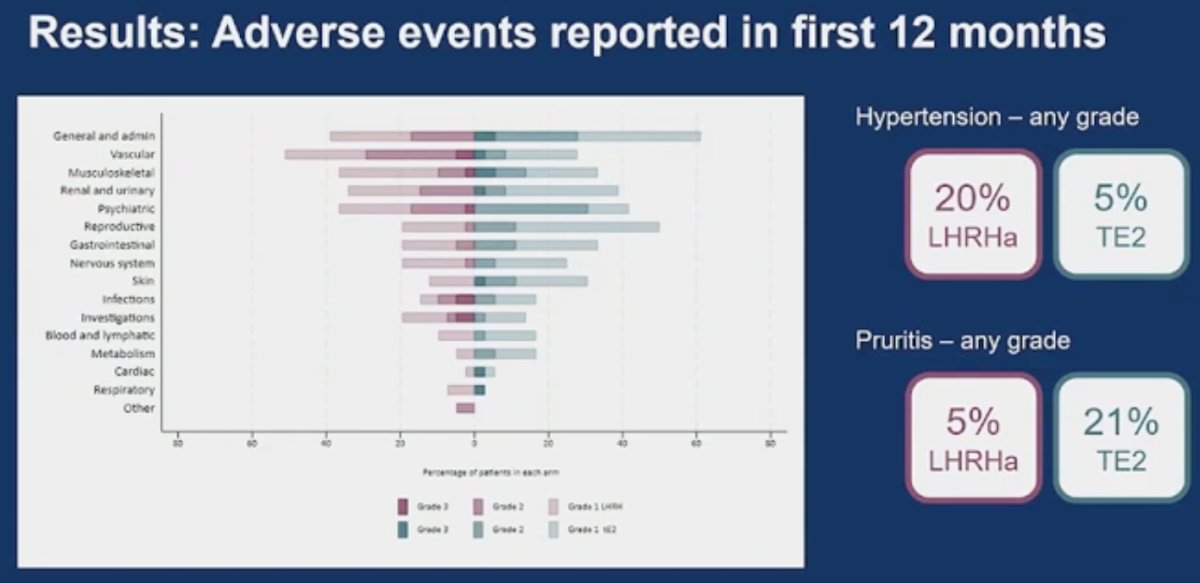
- Adverse events within the first 12 months (including hypertension, hot flushes, and gynaecomastia)
Between October 2020 and March 2023, 79 patients with histologically confirmed M1 prostate cancer received either LHRHa + ARPI (n=41) or transdermal estradiol + ARPI (n=38). The baseline patient characteristics are summarized below. The age at randomization was 69 years. The PSA at randomization was higher in the LHRH agonist group (47 versus 39 ng/mL).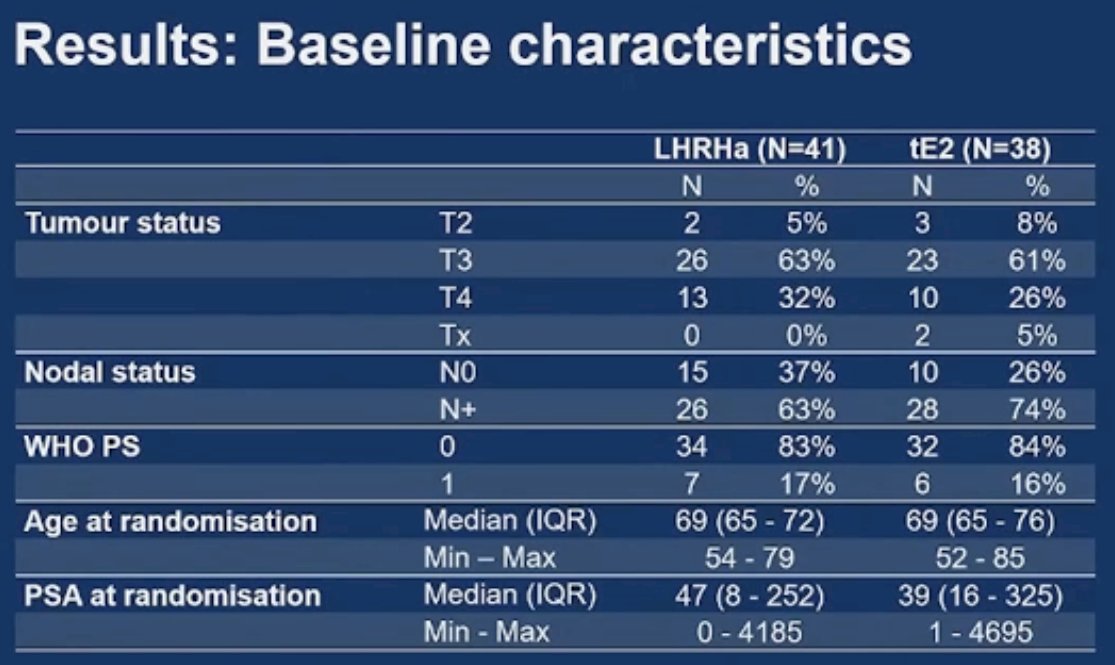
The treatment details are summarized below. He noted an imbalance in the specific ARPI received between the two arms. Most patients (76%) had not received an LHRH agonist previously, with the remaining 24% having received one dose only. The time from randomization to starting ADT or an ARPI was short.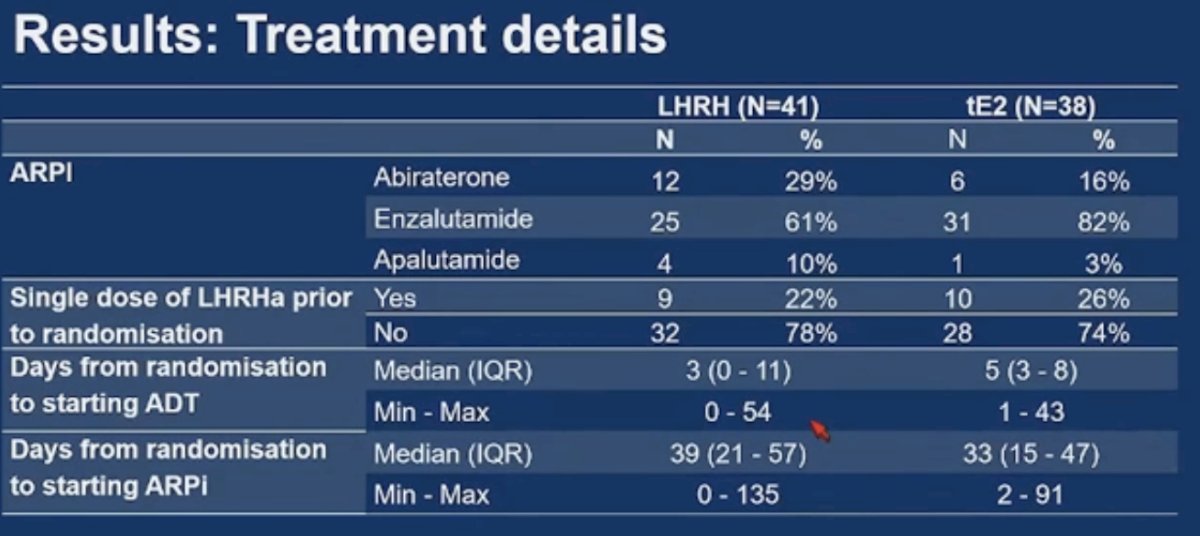
With regards to the primary outcome, the proportion of patients achieving a PSA ≤0.2 ng/mL was 61% in both arms.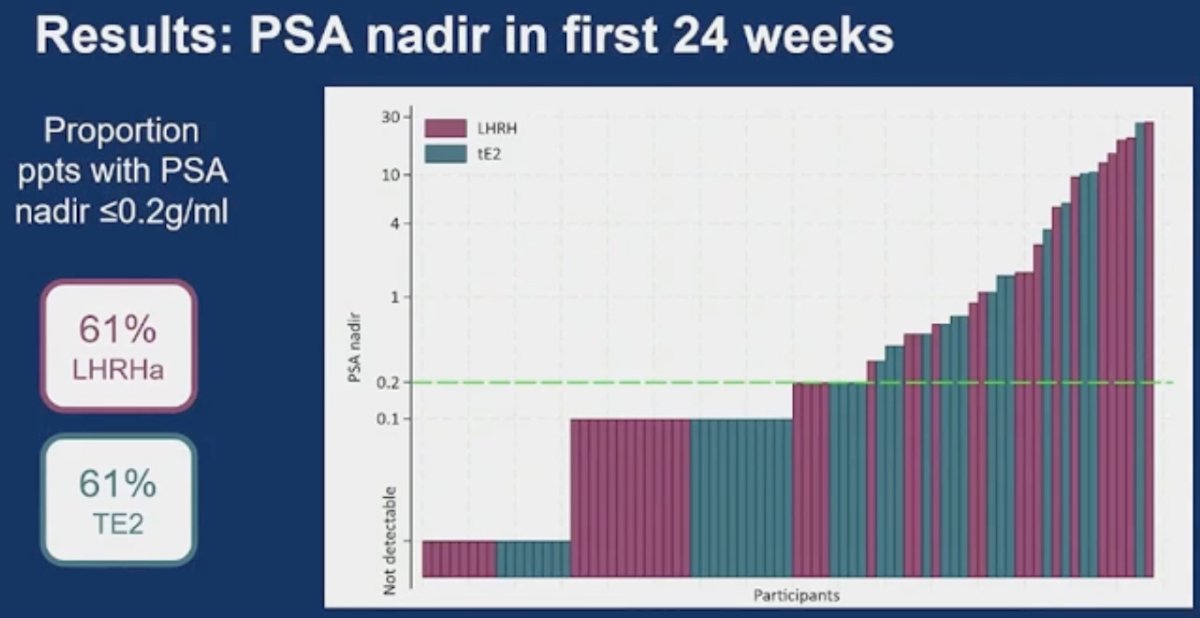
Overall, the incidence of adverse events was similar. However, patients receiving transdermal estrogens were less likely to have any-grade hot flashes (18% versus 54%) or hypertension (5% versus 20%), but more likely to experience any-grade gynecomastia (45% versus 10%) or pruritis (21% versus 5%).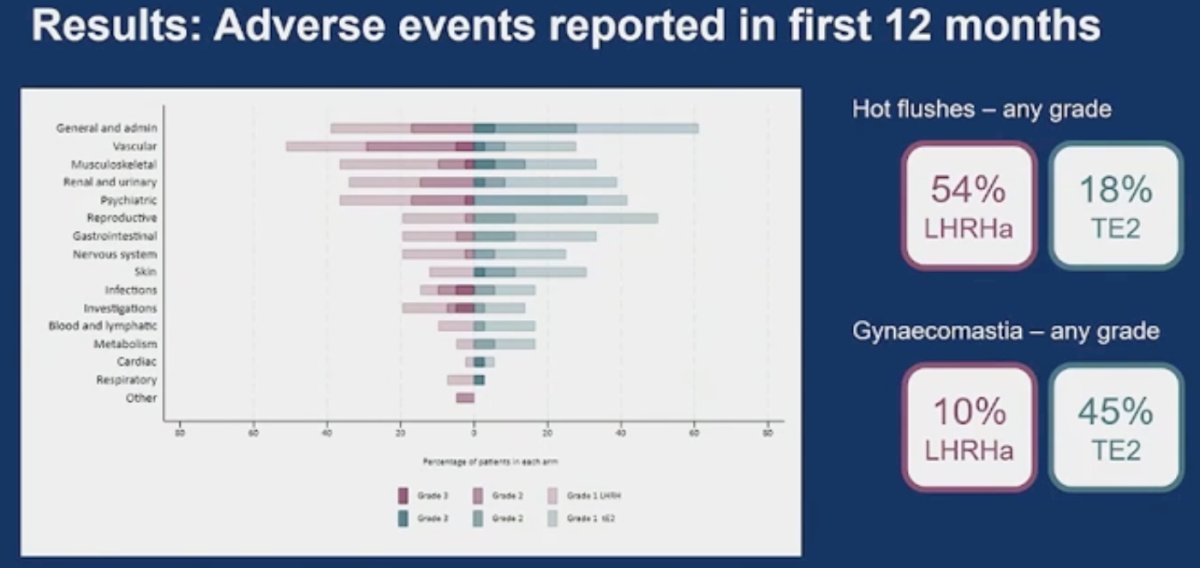
Dr. James noted the following limitations/study considerations:
- This study had a small sample size with relatively short follow-up
- It was difficult to separate difference in responses that may be associated with different ARPIs
- Men were randomized to receive transdermal estradiol or LHRH agonists, but it was the physician’s choice as whether to treat with ARPI and which ARPI, specifically
Dr. James concluded as follows:
- The combination of transdermal estradiol + ARPI is effective
- A similar proportion of men with metastatic HSPC treated with transdermal estradiol +ARPIs achieved a good PSA response, compared to those treated with ARPI + LHRH analogue
- Transdermal estradiol + ARPI is safe
- No new safety signals emerged in men treated with transdermal estradiol + ARPI combination
- Transdermal estradiol represents a viable alternate strategy for ADT giving men more choices
Presented by: Nicholas James, MBBS, PhD, Professor of Prostate and Bladder Cancer Research at The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust, London, UK
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: Estrogen Patches Combined with AR Pathway Inhibitors Show Promise in Prostate Cancer Management - Nicholas James