(UroToday.com) The 2026 ASCO annual meeting featured a kidney cancer session and a presentation by Dr. Eric Martin discussing an artificial intelligence-augmented analysis of quantitative ctDNA burden and longitudinal kinetics to identify prognostic risk stratification in metastatic clear cell renal cell carcinoma (RCC). ctDNA enables minimally invasive monitoring of tumor biology and treatment response; however, its utility in RCC has not been well established. Thus, Dr. Martin and colleagues sought to understand the relationship between ctDNA, tumor histology, and clinical outcomes in locally advanced RCC and metastatic RCC. Furthermore, they applied artificial intelligence–based analysis of quantitative ctDNA trajectories to identify prognostically informative patterns beyond baseline detection.
Overall, 48 patients with locally advanced RCC and metastatic RCC underwent serial plasma ctDNA testing with a commercially available, tumor-informed assay (Signatera). There were 33 patients with metastatic clear cell renal cell carcinoma analyzed who were undergoing longitudinal tumor-informed ctDNA testing during first line immune checkpoint inhibitor based therapy. Survival and response analyses included longitudinal ctDNA profiling. Quantitative ctDNA burden in mean tumor molecules per milliliter (MTM/mL) was measured serially and aligned to treatment initiation, with radiographic response classified as complete response, partial response, stable disease, or progressive disease. ctDNA trajectory similarity was independently assessed using dynamic time warping (DTW), trajectory-based K-means clustering, and a neural network sequence autoencoder (TensorFlow) with clustering to learn latent representations of ctDNA kinetics. Additionally, cross-method concordance was used to define robust ctDNA kinetic phenotypes.
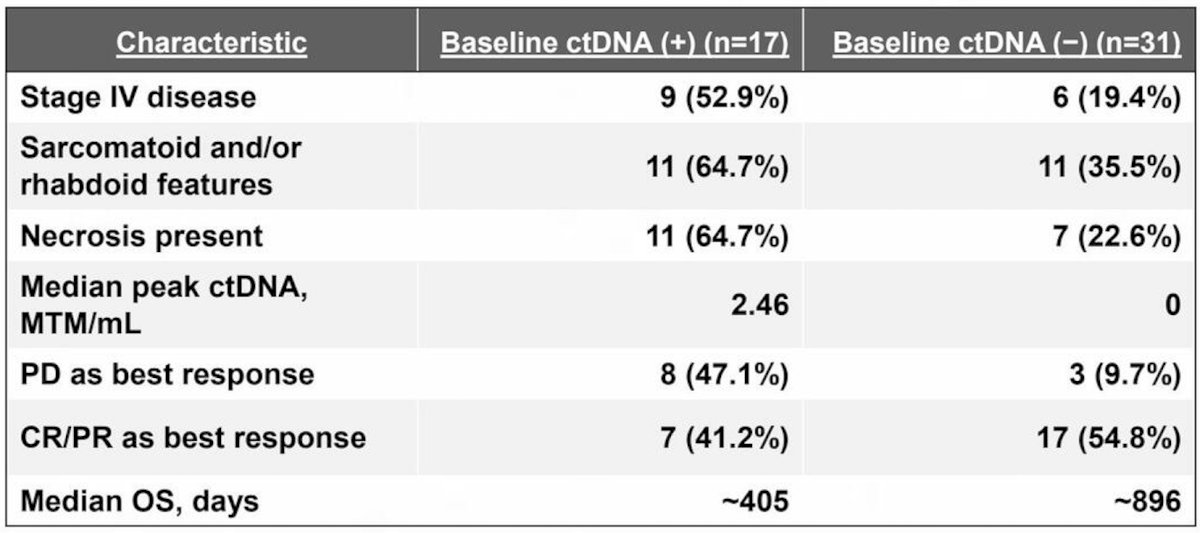
Baseline ctDNA was detected in 39.5% (17/48) of patients overall, including 5.2% (1/19) with locally advanced renal cell carcinoma RCC and 55.2% (16/29) with metastatic renal cell carcinoma:
The following figure shows representative ctDNA trajectories over time for the 33 patients with metastatic clear cell renal cell carcinoma with longitudinal ctDNA profiling:

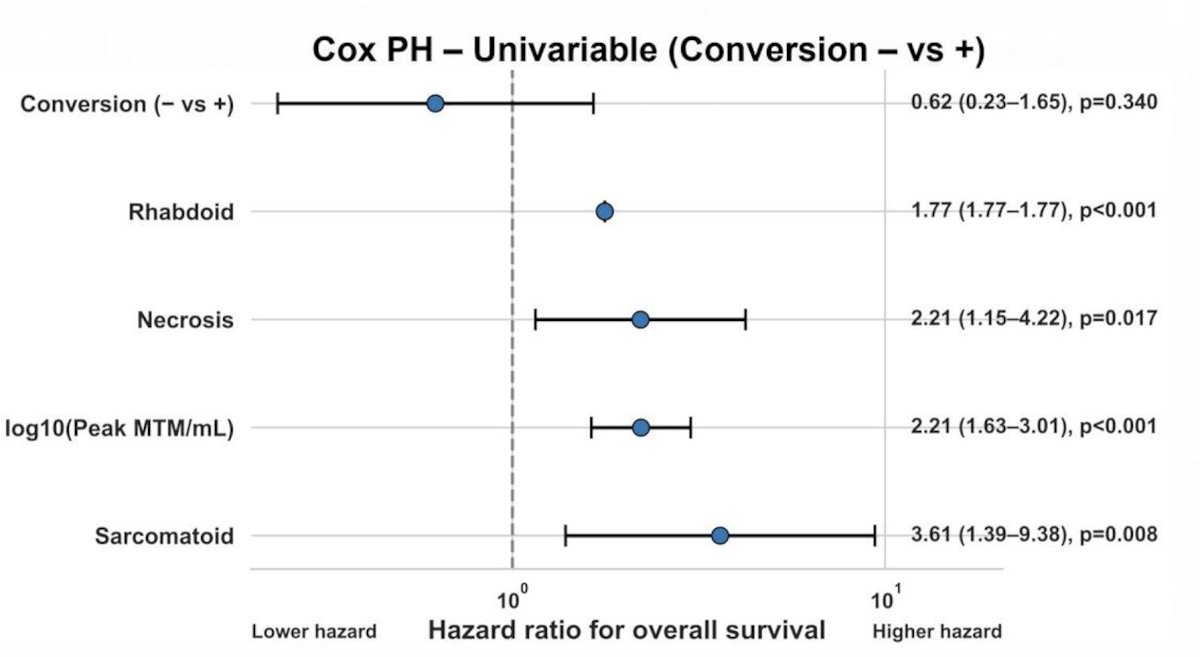
Conversion from ctDNA-positive to ctDNA-negative status during therapy was associated with improved overall survival (p = 0.014), baseline ctDNA detectability was not significantly associated with overall survival:

Increasing peak ctDNA burden was strongly associated with inferior overall survival (HR 2.21, 95% CI 1.63–3.01; p < 0.001). A machine learning-based spline-regularized Cox survival model identified a high-risk ctDNA threshold >20 MTM/mL associated with worse overall survival (p = 0.034):
Longitudinal ctDNA analysis identified four reproducible kinetic phenotypes: early ctDNA clearance, delayed ctDNA clearance, persistently low-level ctDNA, and early/rising ctDNA. Phenotypes were reproducible across K-means clustering, dynamic time warping (DTW), and autoencoder-based modeling:
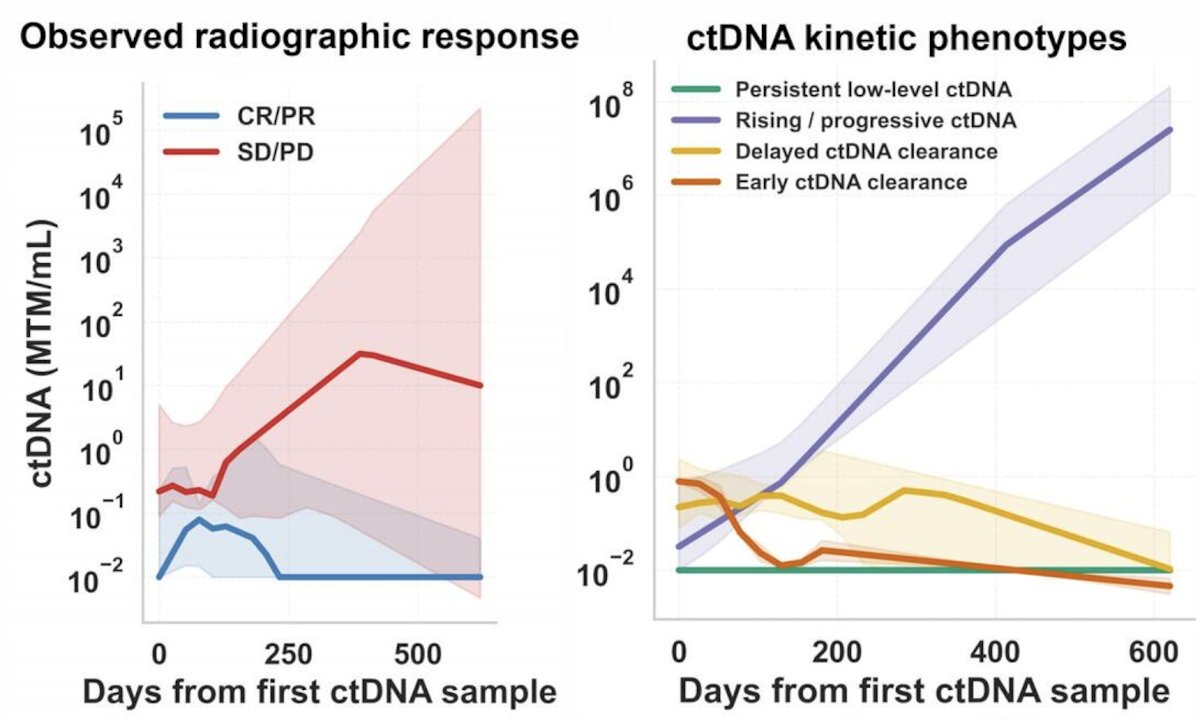
Finally, ctDNA kinetic phenotypes demonstrated distinct radiographic response and survival outcomes, with early/rising ctDNA associated with inferior overall survival (p = 0.022):

Dr. Martin concluded his presentation discussing an artificial intelligence-augmented analysis of quantitative ctDNA burden and longitudinal kinetics to identify prognostic risk stratification in metastatic clear cell RCC with the following take home points:
- Tumor-informed ctDNA correlated with aggressive histopathologic features in RCC
- Persistent ctDNA positivity and higher peak ctDNA burden were associated with worse outcomes
- Longitudinal ctDNA kinetics provided prognostic information beyond baseline detectability
- Longitudinal ctDNA kinetic phenotypes outperform static baseline ctDNA detection
- These findings support ctDNA kinetics as a potential dynamic biomarker for treatment monitoring and risk stratification in metastatic clear cell RCC
Presented by: Eric Martin, Inova Schar Cancer Institute, Fairfax, VA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology Genitourinary (ASCO) Annual Meeting held in Chicago, IL between May 29th and June 1st, 2026